

Translate this page into:
Morphology to molecular subtyping: Retrospective study to correlate the molecular subtypes of breast cancer with mammography and ultrasound imaging features
 , Nishita Goyal1, Harini Gnanavel1, V Pavithra2, Leena Dennis Joseph2, Sanjivanee Ujwal Ingole1
, Nishita Goyal1, Harini Gnanavel1, V Pavithra2, Leena Dennis Joseph2, Sanjivanee Ujwal Ingole1
*Corresponding author: Bhawna Dev, Department of Radiology, Sri Ramachandra Institute of Higher Education & Research, Chennai, Tamil Nadu, India. bhawnadev@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dev B, Goyal N, Gnanavel H, Pavithra V, Joseph LD, Ingole SU. Morphology to molecular subtyping: Retrospective study to correlate the molecular subtypes of breast cancer with mammography and ultrasound imaging features. Indian J Breast Imaging. 2025;3:27–38. doi: 10.25259/IJBI_22_2024
Abstract
Objectives
To identify the imaging features of malignant breast masses on mammogram and ultrasound. To correlate the morphological features of these masses with immunohistochemistry markers for different molecular subtypes of breast cancers.
Materials and Methods
A retrospective study was conducted including 192 patients from April 2018 to March 2022. Based on IHC, biopsy-proven breast cancers were divided into 4 subtypes (Luminal A, Luminal B, HER2, and TNBC). Mammogram and Ultrasound features were independently studied according to ACR BI-RADS Lexicon criteria. Statistical analysis was performed using the Chi-square and Fisher’s exact test with significance at p < 0.05.
Results
Luminal A cases are predominantly irregular hypoechoic anti-parallel masses with spiculated margins and posterior acoustic shadowing. Luminal B cases are commonly irregular hypoechoic anti-parallel masses with spiculated or micro-lobulated margins and no specific posterior features. HER2 cases are predominantly irregular heterogeneous anti-parallel masses with micro-lobulated margins, mixed posterior features, and intra-lesional calcifications. TNBC cases are relatively round to oval wellcircumscribed masses with parallel orientation and posterior acoustic enhancement. Lymphadenopathy, Oedema, and duct involvement were more commonly seen in HER2 and TNBC subtypes. A distinctive feature in our study was a cystic component within TNBC.
Conclusion
Each molecular subtype of breast cancer has certain unique morphological features on imaging that can be used to aid the diagnosis and management of breast carcinoma.
Keywords
Breast cancer
IHC
Malignant breast masses
Molecular subtyping
Morphology

INTRODUCTION
Breast cancer is one of the leading causes of morbidity and mortality among females. With increasing awareness about breast cancer, the number of patients presenting with breast symptoms such as mastalgia, palpable lump, nipple discharge, etc. has also increased. Current-day breast imaging is not only limited to benign-malignant differentiation based on American College of Radiology (ACR) Breast Imaging Reporting and Data Systems (BI-RADS) guidelines but also includes molecular profiling, which is essential for personalized treatment strategies and guided diagnostic and therapeutic procedures.[1]
Histopathological examination (HPE) and immunohisto-chemical analysis have been indispensable prerequisites for breast cancer treatment. However, tumor heterogeneity, such as mosaicism and variability in receptor status across multifocal or multicentric lesions, poses a significant challenge. Thus, image-based prediction may help in deciding if more than one lesion should be biopsied. Additionally, especially for HER2neu status, imaging-based subtyping may help us in deciding if fluorescence in situ hybridization is necessary for confirmation for receptor status. Moreover, in the era of machine learning and artificial intelligence, this information may play a significant role in designing appropriate models. Therefore, this study was designed to correlate the morphological features of malignant masses on mammogram (MG) and ultrasound (USG) with immunohistochemical markers for different molecular subtypes.
MATERIALS AND METHODS
The study was approved by the hospital’s Publication Oversee Committee (IEC Number CSP-MED/20/SEP/61/90), and the need for informed consent was waived off in view of the retrospective study design. The data of known breast cancer patients from April 2018 to March 2022 was retrieved from Hospital information system/Picture archiving and communication System (HIS/PACS), and only those patients with complete data sets, including MG, USG and HPE as well as receptor status, were included. The demographic data, MG findings, breast density, and HPE details, including receptor status, were tabulated.
Imaging Analysis
MG were obtained with standard craniocaudal (CC) and mediolateral oblique (MLO) views for each breast using dedicated full-field digital mammography Amulet Fujifilm equipment. Breast USG was performed using a high-resolution linear-array transducer (10–12 MHz on Toshiba APLIO 500 equipment). The imaging features were recorded as per the descriptors mentioned in the ACR-BI-RADS lexicon from the reports available in the reporting database of our department.
Immunohistochemical Analysis
Histological data was also recorded from the archived records. In our setting, an appropriate block undergoes sectioning of the tissue core into 3 μ thickness and immunohistochemical staining using monoclonal antibodies to the ER, PR, HER2, and Ki67%. Based on immunehistochemical (IHC), biopsy-proven breast cancers were divided into four subtypes: Luminal A cancers have ER/PR-positive status with a Ki67 index <14%; Luminal B cancers have ER/PR-positive status with/without HER2-positive status and Ki67 index >14%; HER2 enriched cancers have ER/PR-negative status with HER2-positive status and a Ki67 index >14%; and Triple negative breast cancer (TNBC) cancers have ER/PR/HER2-negative status.
Statistical Analysis
The radiological features and immunohistochemical data among the four subtypes were recorded in Excel format and analyzed with IBM SPSS Statistics for Windows, Version 23.0 (Armonk, NY: IBM Corp.). The chi-square and Fisher’s exact tests with significance at p < 0.05 were used.
RESULTS
In this study, a total of 192 patients were included with an age range of 51–60 years and a mean age of 56 years. Amongst these, 29 patients had Luminal A-type cancer, 82 were Luminal B, 36 had HER2-enriched, and 45 were triple-negative breast cancer. The most frequently observed breast density pattern was ACR category B, characterized by scattered areas of fibroglandular parenchyma.
Tables 1 and 2 represent MG and US features for each molecular subtype, respectively, based on the ACR lexicon criteria.
| Imaging feature |
Luminal A n = 29 |
Luminal B n = 82 |
HER2-enriched n = 36 |
Triple-negative n = 45 |
| Mass | ||||
| Shape | ||||
| Irregular | 25 (86%) | 78 (95%) | 32 (88%) | 28 (62%) |
| Oval | 1 | 0 | 0 | 12 |
| Round | 1 | 2 | 2 | 4 |
| Non-mass like | 2 | 2 | 2 | 1 |
| Margins | ||||
| Spiculated | 20 (69%) | 44 (53%) | 8 | 7 |
| Microlobulated | 3 | 10 | 13 (36%) | 12 |
| Circumscribed | 1 | 0 | 0 | 17 (37%) |
| Obscured | 2 | 3 | 9 | 8 |
| Indistinct | 1 | 23 | 4 | 0 |
| Non-mass like | 2 | 2 | 2 | 1 |
| Density | ||||
| High | 26 (89%) | 72 (88%) | 31 (86%) | 41 (91%) |
| Equal | 1 | 8 | 3 | 3 |
| Non-mass like | 2 | 2 | 2 | 1 |
| Calcifications | ||||
| Distribution | ||||
| Within mass | 7 (24%) | 6 (7%) | 16 (44%) | 9 (20%) |
| Absent | 22 | 74 | 16 | 36 |
| Grouped | - | 1 | 2 | - |
| Segmental | - | 1 | 2 | - |
| Morphology | ||||
| Amorphous | 5 | 3 | 9 | 6 |
| Linear | 1 | 5 | 3 | 3 |
| Coarse | 1 | - | - | - |
| Not applicable | 22 | 74 | 16 | 36 |
| Pleomorphic | - | - | 8 | - |
| Architectural distorsion | ||||
| Present | 21 (72%) | 34 (41%) | 24 (66%) | 15 (33%) |
| Absent | 8 | 48 | 12 | 30 |
| Focality of mass | ||||
| Single | 27 (93%) | 71 (87%) | 27 (75%) | 37 (82%) |
| Multifocal | 1 | 4 | 4 | 3 |
| Multicentric | 1 | 7 | 3 | 3 |
| Bilateral | 0 | - | 1 One with satellite nodule - 1 |
2 |
| Associated features | ||||
| Nipple retraction | 2 (6%) | 13 (15%) | 6 (16%) | 2 (4%) |
| Absent | 27 | 69 | 30 | 43 |
| Skin thickening | 5 (17%) | 24 (29%) | 19 (52%) | 12 (26%) |
| Absent | 24 | 58 | 17 | 33 |
| Lymph node | 13 (44.8%) | 35 (42%) | 26 (72%) | 35 (77%) |
| Absent | 16 | 47 | 10 | 10 |
| Location | ||||
| Laterality | ||||
| Right | 19 | 39 | 21 | 17 |
| Left | 10 | 43 | 15 | 28 |
| Quadrant | ||||
| Upper outer | 13 | 44 | 15 | 24 |
| Upper inner | 4 | 8 | 4 | 6 |
| Lower outer | 3 | 7 | 5 | 2 |
| Lower inner | 4 | 8 | 3 | 3 |
| Central | 5 | 10 | 7 | 5 |
| Remaining | - | 5 | 2 | 5 |
MG: Mammogram, HER2: Human epidermal growth factor receptor 2.
| Imaging feature |
Luminal A n = 29 |
Luminal B n = 82 |
HER2-enriched n = 36 |
Triple-negative n = 45 |
| Mass | ||||
| Shape | ||||
| Irregular | 29 (100%) | 79 (96%) | 34 (94%) | 28 (62%) |
| Oval | - | 2 | - | 5 |
| Non-mass | - | 1 | 2 | - |
| Round | - | - | - | 12 |
| Margins | ||||
| Spiculated | 26 (89%) | 53 (66%) | 6 | 9 |
| Microlobulated | 2 | 19 | 28 (78%) | 19 (42%) |
| Indistinct | 1 | 8 Non mass like - 1 Partly obscured - 1 |
2 | 1 Obscured - 1 Circumscribed - 5 (33%) |
| Orientation | ||||
| Anti-parallel | 28 (97%) | 79 (96%) | 34 (94%) | 28 (62%) |
| Parallel | 1 | 2 | - | 17 |
| Non mass like | - | 1 | 2 | - |
| Echo pattern | ||||
| Hypoechoic | 23 (79%) | 63 (77%) | 7 | 13 |
| Heterogeneous | 6 | 18 Non mass with heterogeneous echoes - 1 |
27 (75%) Isoechoic - 2 | 32 (71%) |
| Posterior features | ||||
| Shadowing | 23 (79%) | 10 | - | 2 |
| Enhancement | 2 | 6 | 8 | 29 (64%) |
| No features | 4 | 54 (66%) | 11 | 13 |
| Mixed | - | 12 | 17 (47%) | 1 |
| Calcifications | ||||
| Present | 5 | 8 | 17 | 11 |
| Absent | 24 | 74 | 19 | 34 |
| Associated features | ||||
| Skin thickening | ||||
| Absent | 5 (17%) 24 |
24 (29%) 58 |
12 (33.3%) 24 |
12 (26.6%) 33 |
| Nipple | ||||
| Retraction | 2 (6%) | 13 (15%) | 5 (13.8%) | 2 (4%) |
| Absent | 27 | 69 | 31 | 43 |
| Lymph node | 13 (44.8%) | 42 (52%) | 26 (72%) | 33 (73.4%) |
| Absent | 16 | 40 | 10 | 12 |
| Cystic component | 0 | 3 | 1 | 14 (31.1%) |
| Edema | 0 | 1 | 4 | 3 |
| Duct | 1 | 2 | 3 | 1 |
US: Ultrasound, HER2: Human epidermal growth factor receptor 2.
Luminal A Breast Cancer
The masses were predominantly irregular (n = 25, 86%) and had spiculated margins (n = 20, 69%), and the majority of masses were classified as high-density (n = 26, 89%) on MG. Associated calcifications were seen in 24% (n = 7) and architectural distortion (AD) in 72% (n = 21) of the masses. Most of the patients had a single mass (93%, n = 27), predominantly in the upper outer quadrant. All the masses were irregular in shape (n = 29, 100%) on US, with the majority having spiculated margins (n = 26, 89%) and anti-parallel orientation (n = 28, 97%).
Luminal B Breast Cancer
The Luminal B breast cancers were predominantly irregularly shaped (n = 78, 95%); had spiculated margins in 53% (n = 44); and were of high density (n = 72, 88%) as compared to fibroglandular parenchyma. Only 7% (n = 6) had calcification within the mass, and 41% (n = 71) had AD. The masses were irregular (n = 79, 96%), spiculated (n = 53, 66%), and anti-parallel (n = 79, 96%) on USG.
HER2-Enriched Breast Cancer
The mass shape was primarily irregular (n = 32, 88%) with microlobulated margins (n = 13, 36%) and associated calcification in 44% (n = 16) and AD in 66% (n = 24) on MG. The masses were mostly located in the upper outer quadrant (n = 15). On USG, this group had irregular masses in 34 patients (94%), and the majority had microlobulated margins (n = 28, 78%). Duct involvement was seen in three cases (8%).
Triple-Negative Breast Cancer
The masses were predominantly irregular (n = 28, 62%) but also had oval (27%, n = 12) and round shapes (9%, n = 4). Circumscribed margins were most common (n = 17, 37%), followed by microlobulated margins in 27% (n = 12) on MG. Calcifications were seen in 20% (n = 9) and AD in 33% (n = 15). The masses had irregular shapes on USG in 28 cases (62%), microlobulated margins in 19 (42%), and circumscribed margins in 15 (33%). Anti-parallel orientation was predominant (n = 28, 62%), but a significant number also showed parallel orientation (n = 17, 38%). Cystic components were observed in 14 cases (31.1%), which is the highest for any subtype.
Comparative Evaluation of Different Molecular Subtypes
Mammographic Findings
Spiculated margins were common in Luminal A and Luminal B (p < 0.005), whereas HER2-enriched showed a significantly higher number of masses with microlobulated margins (p < 0.002), and TNBC had a higher frequency of circumscribed margins (p < 0.002).Calcifications were more likely to be associated with HER2-enriched (44%) and TNBC (20%) (p < 0.002). Nipple retraction was more frequent in Luminal B (15%) and HER2-enriched subtypes (16%) (p = 0.47). Lymph node involvement was most common in HER2-enriched (72%) and triple-negative subtypes (77%), with USG being better at detecting this feature, identifying it in 72% of HER2-enriched and 73.4% of TNBC cases (p = 0.41).
USG Findings
Across all subtypes, irregular mass shape was the most frequent finding on USG. Spiculated margins were most common in Luminal A and Luminal B (89% and 66%, respectively), but circumscribed margins were more common in triple-negative cancers (33%). Anti-parallel orientation was observed in most cases across all subtypes, highest in Luminal A (97%).
Hypoechoic masses were most common in Luminal A and Luminal B (79% and 77%, respectively), while heterogeneous echo patterns were more common in HER2-enriched and triple-negative cancers (75% and 71%, respectively). Skin thickening was present in all subtypes, with the highest seen in HER2-enriched tumors (33.3%). Lymph node involvement was most frequently seen in HER2-enriched and triple-negative subtypes (72% and 73.4%, respectively). Cystic components were most often found in triple-negative cancers (31.1%).
No significant correlation was found for vascularity, the focality of mass, and quadrant location of the breast masses among different molecular subtypes on imaging.
For the HER2-enriched subtype, the typical USG features included an irregular shape, micro-lobulated margins, and mixed posterior features. These were present in 8 out of 36 HER2 cases (22.2%), while only 4 out of 156 cases (2.6%) in other subtypes showed these characteristics (p < 0.002). In the triple-negative breast cancer subtype, the most common USG features were an oval shape, circumscribed margins, and posterior enhancement. These features were observed in 7 out of 45 TNBC cases (15.6%), while 1 out of 147 cases (0.7%) in other subtypes displayed similar characteristics (p < 0.002).
DISCUSSION
Over the last decade, the focus of diagnosing breast cancer has shifted from histopathological examination (HPE) alone to combined HPE and IHC analysis. Hormonal and oncogene-targeted therapies are important steps in the management of patients as part of preoperative planning or even for non-resectable metastatic tumors as palliative treatment. Hence, the contribution of radiologists is to aid in the diagnosis and management of such patients by identifying the unique features of imaging in each type.
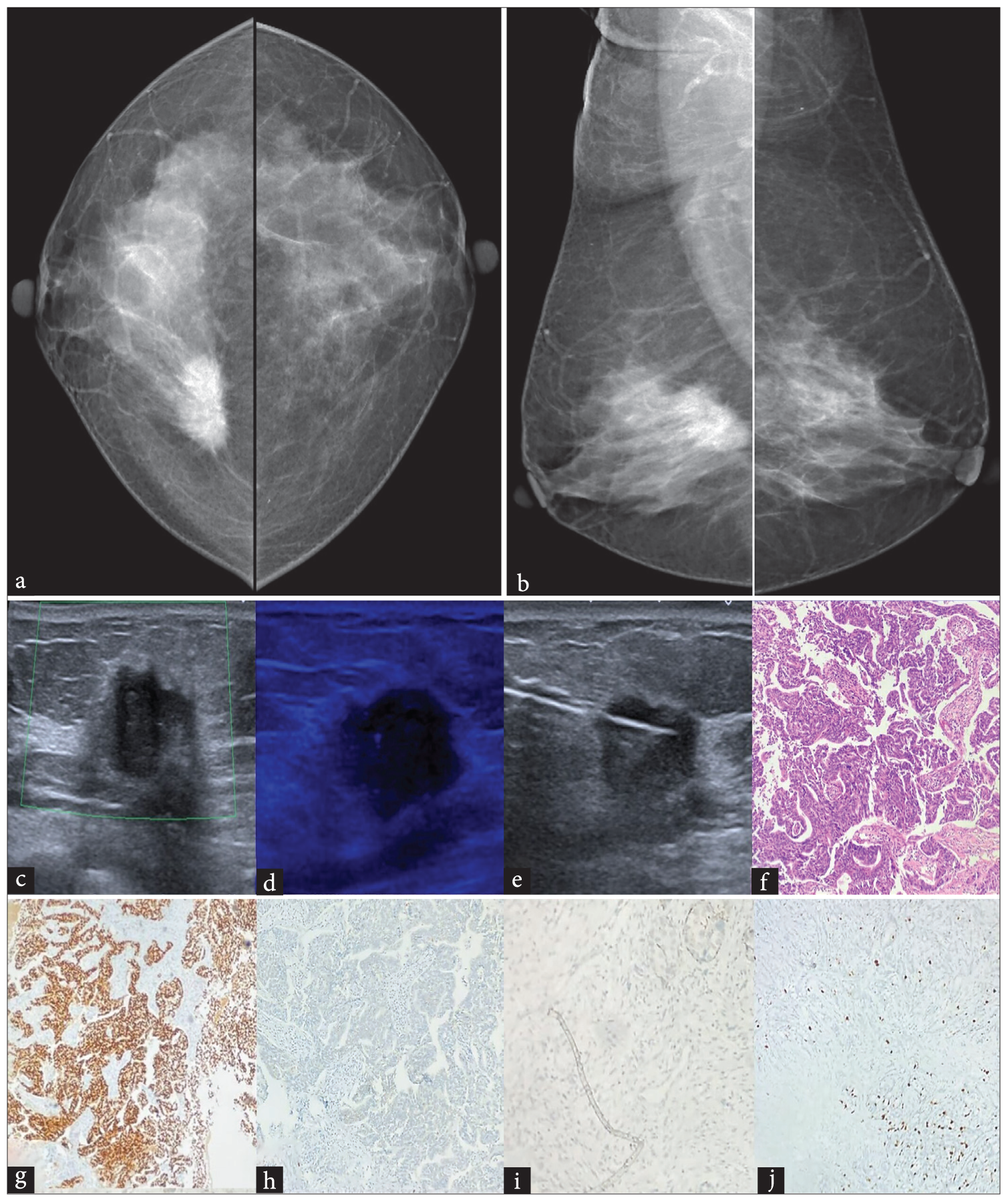
In our study, Luminal A cases most commonly presented as irregular, spiculated masses on MGs [Figure 1a and 1b] and appeared hypoechoic and antiparallel on USG with posterior acoustic shadowing [Figure 1c]. AD was observed more frequently in this subtype, although the difference was not statistically significant. Our findings were in concordance with the other studies, which suggested that most Luminal type A masses had spiculated margins and more frequent association with AD as compared to other subtypes.[2–10] We observed that microcalcifications were less common in Luminal A (24%) compared to other subtypes, which is in discordance with a study done by Cen et al., who reported grouped or clustered calcifications in 70% of hormone receptor-positive cancers.[11] Similarly, studies by Rashmi et al. and Mi Young Kim et al. described the presence of coarse heterogeneous calcifications in Luminal A subtypes.[12,13]

- Luminal A breast cancer: Mammogram (a) CC and (b) MLO views of a 50-year-old female with Type B breast parenchyma show an irregular high-density mass with spiculated margins in upper central quadrant of the right breast with nipple retraction. No significant right axillary lymph adenopathy. (c) US shows an irregular anti-parallel oriented hypo-echoic mass with spiculated margins and posterior acoustic shadowing in the sub-areolar region of the right breast. (d) Increased internal vascularity is seen within. (e) No significant lymph nodes are seen in the right axilla. (f) Histopathology shows invasive mammary carcinoma- Nottingham histological grade II (H&E x 100). Tumor cells showing (g) ER positivity, (h) PgR positivity, (i) HER2 negativity (j) and Ki67 index <14 % (IHC x100). CC: Cranio-caudal, MLO: Mediolateral oblique, US: Ultrasound, H&E: Hematoxylin and eosin, ER: Estrogen receptor, PgR: Progesterone receptor, HER2: Human epidermal growth factor receptor 2, IHC: Immunohistochemistry.
6% cases showed nipple retraction compared to Luminal B and HER2 enriched breast cancer [Figure 1d]. Luminal A cases in our study had fewer number of patients with axillary lymph adenopathy compared to other subtypes [Figure 1e]. Representative Figure 1f–j shows pathological findings for Luminal A mass which was invasive mammary cacinoma on histology with ER, PgR positivity, HER2 negativity and Ki67% index <14% on IHC.
In Luminal B, the masses were predominantly irregular in shape, spiculated, and exhibited high density on mammography. This aligns with the findings of Algazzar et al., who reported that 100% of Luminal B lesions in their study were irregular in shape.[14] On USG also, 96.3% (n = 79) of masses were irregular in shape, similar to 76.7% of irregular Luminal B masses in a study by Boisserie-Lacroix et al.[2] In this study, 53% of cases (n = 44) of Luminal B demonstrated spiculated margins [Figure 2a and b], and 28% of cases exhibited indistinct margins, a finding consistent with the results reported by Tong Wu et al.[8] Nearly 96% (n = 79) of the masses identified on USG were anti-parallel in our study [Figure 2c], similar to the study by Shaikh et al. and Khalaf et al.[3,6] 77% (n = 63) of masses were hypoechoic in our study, similar to the findings documented by Boisserie-Lacroix et al.[2] A significant number of patients in this group showed AD, which is in line with observations made by Wojcinski et al.[15] Calcifications, although less frequent, were primarily intralesional. Among these, fine linear and amorphous patterns were the most commonly observed, suggestive of malignancy, (Figure 2d US image showing no calcification within mass), which is similar to the findings described by Cen et al.[11] Focal asymmetry was an uncommon feature, in agreement with the observations made by Ian et al.[5] Tru-cut biopsy is required for pathological analysis due to suspcious imaging features [Figure 2e]. Representative Figure 2f–j shows pathological findings for Luminal B mass which was invasive mammary cacinoma on histology with ER, PgR positivity, HER2 negativity and Ki67% index >14% on IHC.
- Luminal B breast cancer: Mammogram (a) CC and (b) MLO views of a 53-year-old female with Type B breast parenchyma showing an irregular high-density mass with spiculated margins in central inner quadrant of the right breast. (c) US shows an irregular anti-parallel oriented heterogeneously hypoechoic mass with angular margins and posterior shadowing in the right breast with no significant internal vascularity. (d) No calcifications seen within. (e) US guided Tru-cut biopsy image of the right breast mass. (f) Histopathology shows invasive mammary carcinoma, no special type, with islands of tumor cells. (H&E x 100). Tumor cells showing (g) ER positivity, (h) PgR positivity, (i) HER2 negativity and (j) Ki67 index >14 % (IHC x100). CC: Cranio-caudal, MLO: Mediolateral oblique, US: Ultrasound, H&E: Hematoxylin and eosin, ER: Estrogen receptor, PgR: Progesterone receptor, HER2: Human epidermal growth factor receptor 2, IHC: Immunohistochemistry.
The HER2-enriched subtype typically presented as irregular, high-density masses on mammography [Figure 3a and b], a finding supported by previous studies.[14,16] Margins were frequently micro-lobulated and non-circumscribed, consistent with observations reported by Wojcinski et al.[15] This group had the highest incidence of calcifications among all subtypes, with [Figure 3a and b]. Among 20 cases, 16 (80%) exhibited intralesional calcifications. Amorphous calcifications were the most common, observed in 45% (n = 9) of patients, followed by fine pleomorphic calcifications in 40% (n = 8). These findings are in alignment with a study done by Cen et al., who reported amorphous or coarse heterogeneous calcifications in 56.5% of HER2-positive cases.[11] However, other studies have also indicated an association of linear or linear branching calcification patterns with HER2-enriched tumors.[4,17] On USG, 94% of cases appeared as irregular masses [Figure 3c], a finding that is in agreement with previously published studies.[2,4,5] In contrast, Ḉelebi et al. reported that 55% of HER2-positive masses were circumscribed, highlighting variability in USG characteristics.[10] We also found that nearly 97% (n = 28) of HER2-enriched masses were arranged in an anti-parallel orientation on USG [Figure 3c], consistent with earlier reports.[3,6–8,18] In our study, nearly 72% HER2 cases had associated axillary lymphadenopathy [Figure 3d], which was concordant with the results of study by Khalaf et al.[6] Tru-cut biopsy is performed for H&E and IHC analysis for molecular subtyping [Figure 3e]. Representative Figure 3f–j shows pathological findings for HER2 Enriched mass which was invasive mammary cacinoma on histology with ER and PgR negativity, HER2 positivity, and Ki67% index 20% on IHC.

- HER2 Enriched breast cancer: Mammogram (a) CC and (b) MLO views of a 47-year-old female with Type B breast parenchyma showing an irregular high-density mass with micro-lobulated margins in upper outer quadrant of the right breast. Amorphous microcalcifications are seen within the mass. Mild diffuse skin thickening noted. (c) US shows an irregular anti-parallel oriented heterogeneously hypoechoic mass with micro-lobulated margins and few calcifications in the right breast. (d) Few enlarged lymph nodes with increased cortical thickness and loss of fatty hilum are seen in the right axilla. (e) US guided Tru-cut biopsy image of the right breast mass. (f) Histopathology shows invasive mammary carcinoma with a focal micropapillary pattern. (H&E x 100). Tumor cells with (g) ER negativity, (h) PgR negativity, (i) HER2 positivity and (j) Ki67 index 20 % (IHC x100). CC: Cranio-caudal, MLO: Mediolateral oblique, US: Ultrasound, H&E: Hematoxylin and eosin, ER: Estrogen receptor, PgR: Progesterone receptor, HER2: Human epidermal growth factor receptor 2, IHC: Immunohistochemistry.
TNBC in our study commonly presented as irregular or round-to-oval masses, consistent with findings reported by previous studies.[7,14,19–25] Circumscribed margins were frequently observed [Figure 4a and b], a feature also studied by Cho et al., who found that TNBC masses often demonstrate more circumscribed borders.[4] Approximately 38% (n = 17) of the masses in our study exhibited parallel orientation [Figure 4c], aligning with the literature.[7,20] AD was observed in 33% of cases, in contrast to the study by Ian et al., which reported no significant presence of this feature.[5]Masses were heterogeneously hypoechoic in our study on USG, whereas a hypoechoic echo pattern is the most commonly described feature of TNBC.[7,8,16,19,24,25] Although 24% of patients showed intralesional calcifications on USG, Ko et al.[20] and Dogan et al.[23] did not find any significant calcifications in TNBC masses on USG.[19,20] Nearly 31% of cases had a cystic component within masses on USG imaging [Figure 4d] which may be attributed to the higher grade of these tumors. Schopp et al.[21] has also suggested the appearance of TNBC masses as complex solid cystic masses and mimicking benign cystic entities.[21] Skin thickening was seen in 26% of TNBC; however, Evans et al.[19] reported that skin thickening has limited prognostic value in triple-negative breast cancer relative to other subtypes.[22] TNBC cases also showed a higher incidence of lymph node involvement, corroborating with the findings of Evans et al.[19], Tandon et al.[7] found a notable portion of TNBC cases with lymph node involvement, while Cen et al.[11] observed a lower incidence, and San-Gang Wu et al.[26] reported an even smaller proportion.[7,11,23] This variation suggests that the hematogenous route of metastasis might be more common in high-grade TNBC tumors compared to lymph nodal spread. Representative Figure 4e–i shows pathological findings for Triple-negative breast mass which was invasive mammary cacinoma on histology with ER, PgR and HER2 negativity with Ki67% index 45% on IHC.

- Triple-negative breast cancer: Mammogram (a) CC and (b) MLO views of a 60-year-old female with Type A breast parenchyma showing an oval high-density mass with circumscribed margins in the subareolar region of the right breast. Two focal microcalcifications are seen within the lesion. Popcorn calcification is seen in the upper central quadrant of the right breast posterior to the aforementioned mass and within two high-density masses seen in the upper outer and lower inner quadrant respectively in the left breast– suggestive of involuting fibroadenoma. (c) US shows an oval circumscribed heterogeneously hypoechoic mass with posterior acoustic enhancement in the subareolar region of the right breast. (d) Mild internal vascularity and cystic components are seen in the mass. (e) Histopathology shows invasive mammary carcinoma, no special type. (H&E x 100). Tumor cells with (f) ER negativity, (g) PgR negativity, (h) HER2 negativity and (i) Ki67 index 45 % (IHC x100). CC: Cranio-caudal, MLO: Mediolateral oblique, US: Ultrasound, H&E: Hematoxylin and eosin, ER: Estrogen receptor, PgR: Progesterone receptor, HER2: Human epidermal growth factor receptor 2, IHC: Immunohistochemistry.
Although this study is limited by small sample size and retrospective design from a single institute, it has highlighted the role of IHC correlation with imaging markers, which may assist in further prospective validation studies. This study demonstrated Luminal A to have predominantly irregular masses with spiculated margins and posterior acoustic shadowing; Luminal B as irregular masses with spiculated or micro-lobulated margins and no specific posterior features; and HER2-enriched tumors as predominantly irregular masses with micro-lobulated margins, mixed posterior features, and intra-lesional calcifications. TNBC cases were relatively round to oval, well-circumscribed masses with parallel orientation and posterior acoustic enhancement.
CONCLUSION
To conclude, a diligent approach in interpreting suspicious breast masses on MGs and USGs according to the ACR-BI-RADS 5th edition Lexicon shall lead to the correct interpretation and correlation of imaging with molecular subtypes of breast cancer in concordance with gold standard IHC biomarkers.
Ethical approval
The research/study was approved by the Institutional Review Board at Sri Ramachandra Institute of Higher Education & Research, number CSP-MED/20/SEP/61/90, dated September 2020.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- American College of Radiology. [Last accessed 29 September 2024]. Available from: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads
- [Google Scholar]
- Triple-negative breast cancers: Associations between imaging and pathological findings for triple-negative tumors compared with hormone receptor-positive/human epidermal growth factor receptor-2-negative breast cancers. Oncol. 2013;18:802-11.
- [Google Scholar]
- Predicting molecular subtypes of breast cancer with mammography and ultrasound findings: Introduction of sono-mammometry score. Radiol Res Pract. 2021;2021:6691958.
- [Google Scholar]
- Molecular subtypes and imaging phenotypes of breast cancer. Ultrason Seoul Korea. 2016;35:281-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Role of mammogram and ultrasound imaging in predicting breast cancer subtypes in screening and symptomatic patients. World J Clin Oncol. 2021;12:808-22.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Role of ultrasound in predicting the molecular subtypes of invasive breast ductal carcinoma. Egypt J Radiol Nucl Med. 2020;51:138.
- [Google Scholar]
- Role of sonography in predicting the hormone receptor status of breast cancer: A prospective study. J Diagn Med Sonogr. 2018;34:3-14.
- [Google Scholar]
- Identification of a correlation between the sonographic appearance and molecular subtype of invasive breast cancer: A review of 311 cases. Clin Imaging. 2019;53:179-85.
- [CrossRef] [PubMed] [Google Scholar]
- Assessing the role of ultrasound in predicting the biological behavior of breast cancer. Am J Roentgenol. 2013;200:284-90.
- [CrossRef] [PubMed] [Google Scholar]
- The role of ultrasonographic findings to predict molecular subtype, histologic grade, and hormone receptor status of breast cancer. Diagn Interv Radiol Ank Turk. 2015;21:448-53.
- [Google Scholar]
- BI-RADS 3–5 microcalcifications can preoperatively predict breast cancer HER2 and Luminal a molecular subtype. Oncotarget. 2017;8:13855-62.
- [Google Scholar]
- Predicting the molecular subtype of breast cancer based on mammography and ultrasound findings. Indian J Radiol Imaging. 2018;28:354-61.
- [Google Scholar]
- Mammographic and ultrasonographic features of triple-negative breast cancer: A comparison with other breast cancer subtypes. Acta Radiol. 2013;54:889-94.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Breast cancer imaging features as a predictor of the hormonal receptor status, HER2neu expression and molecular subtype. Egypt J Radiol Nucl Med. 2020;51:93.
- [Google Scholar]
- Sonographic features of triple-negative and non-triple-negative breast cancer. J Ultrasound Med. 2012;31:1531-41.
- [CrossRef] [PubMed] [Google Scholar]
- Estrogen receptor-negative invasive breast cancer: Imaging features of tumors with and without human epidermal growth factor receptor type 2 overexpression. Radiology. 2008;246:367-75.
- [CrossRef] [PubMed] [Google Scholar]
- Mammographic features of calcifications in DCIS: correlation with oestrogen receptor and human epidermal growth factor receptor 2 status. Eur Radiol. 2013;23:2072-8.
- [Google Scholar]
- Identifying ultrasound and clinical features of breast cancer molecular subtypes by ensemble decision. Sci Rep. 2015;5:11085.
- [Google Scholar]
- The value of prognostic ultrasound features of breast cancer in different molecular subtypes with a focus on triple negative disease. Breast Cancer. 2022;29:296-301.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Triple-negative breast cancer: Correlation between imaging and pathological findings. Eur Radiol. 2010;20:1111-7.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging challenges in diagnosing triple-negative breast cancer. RadioGraphics. 2023;43:e230027.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging features of breast cancer subtypes on mammography and ultrasonography: An analysis of 479 patients. Indian J Surg Oncol.. 2022;13:931-8.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Multimodality imaging of triple receptor-negative tumors with mammography, ultrasound, and MRI. Am J Roentgenol. 2010;194:1160-6.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of ultrasound findings with histology, tumor grade and biological markers in breast cancer. Acta Oncol Stockh Swed. 2008;47:1531-8.
- [CrossRef] [PubMed] [Google Scholar]
- Ultrasonographic features of triple-negative breast cancer: A comparison with other breast cancer subtypes. Asian Pac J Cancer Prev. 2015;16:3229-32.
- [Google Scholar]
- Prognostic value of metastatic axillary lymph node ratio for chinese breast cancer patients. PLoS One. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0061410
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




