

Translate this page into:
Case report of a rare benign breast lesion: Unveiling nipple adenoma

*Corresponding author: Raunak Sinha, Department of Radiodiagnosis, All India Institute of Medical Sciences, Phulwarisharif, Patna, India. drraunaksinha@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sinha U, Sinha R, Sinha R, Haq A. Case report of a rare benign breast lesion: Unveiling nipple adenoma. Indian J Breast Imaging. 2024;2:29-33. doi: 10.25259/IJBI_15_2023
Abstract
Nipple adenoma is a rare and benign proliferative lesion originating from the lactiferous ducts of the nipple. It predominantly affects middle-aged women and can mimic the clinical and radiological features of more concerning breast malignancies. Due to its uncommon occurrence and overlapping characteristics with malignant lesions, a definitive diagnosis often requires histopathological examination. We present a case of nipple adenoma in a 30-year-old woman, detailing the clinical, radiological, and histopathological features, as well as the management and outcomes.
Keywords
Nipple adenoma
Lactiferous duct
Paget’s disease
Nipple eczema

INTRODUCTION
Nipple adenoma is a rare benign epithelial tumor of the lactiferous duct, accounting for just 0.1–1.7% of benign breast lesions.[1] Clinically, patients present with a unilateral palpable or visible nodule in the nipple with friable tissue with or without erythema, or they may be clinically occult. There can be nipple erosion or focal ulceration with resultant bleeding that may be perceived as bloody nipple discharge, with exudative crustation that mimics eczematoid changes, as seen in Paget disease or nipple eczema. The lesions are often mammographically occult while appearing as hypervascularly circumscribed masses with variable echogenicity on ultrasound (US). Histologically, they are characterized by the proliferation of tubular and glandular structures within the stroma. Despite its benign nature, nipple adenoma causes concern for malignancy, clinically necessitating further investigation and diagnostic confirmation.
CASE REPORT
A 30-year-old female presented to our outpatient department (OPD) with nipple ulceration of the left breast. The patient was relatively asymptomatic four years back when she first noticed a tiny swelling over the lateral aspect of her left nipple. She accidentally scratched the area, which healed with a scab formation. The scab peeling off exposed a purplish wound that remained static for a year. Then, she developed a reddish wound that deepened to its final size. Meanwhile, she was diagnosed and treated for eczema. Both the axillae and right breast were normal. There was no history of fever, swelling of the left breast, nipple discharge, or pain in the nipple region.
On clinical examination, it was found that the left nipple was enlarged in size as compared to the right side, with a 7 × 5 mm irregular, well-defined ulcer over the lateral aspect of the left nipple. Bleeding from the ulcer was noted.
Mammography was not done, considering her young age. The ultrasound revealed an isoechoic mass with an indistinct margin located eccentrically in the nipple and extensive vascularity in the entire lesion [Figure 1]. On Magnetic Resonance Imaging (MRI), a relatively circumscribed lesion was seen within the nipple, predominantly involving the lateral half of the nipple, appearing as intermediate signal intensity on T1WI and heterogeneously hyperintense on T2WI and Short Tau Inversion Recovery (STIR) [Figure 2]. The mass showed intense post-contrast enhancement with a type 2 kinetic curve on dynamic T1 fat-saturated sequences [Figures 3 and 4]. Posteriorly, the lesion was seen involving the base of the nipple.
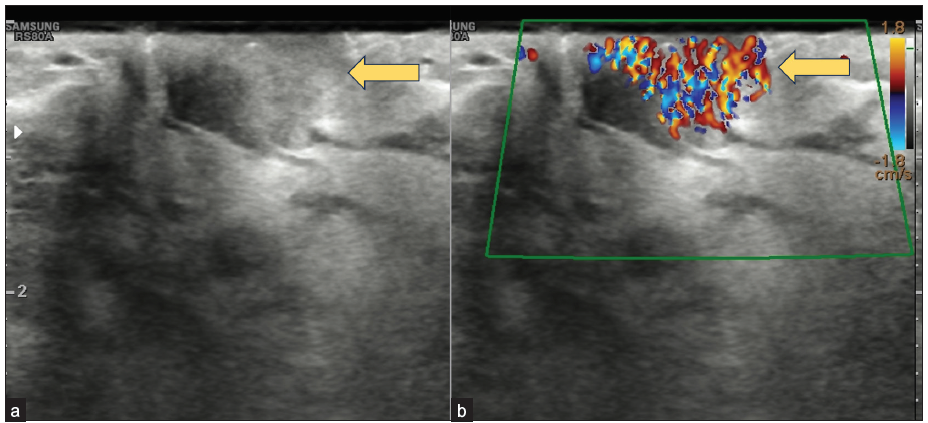
- Transverse ultrasound of the left nipple: (a) an isoechoic 1.8 × 1.6 cm, ovoid mass with indistinct margins within the left nipple (yellow arrow), with (b) extensive internal vascularity (yellow arrow) on color Doppler.
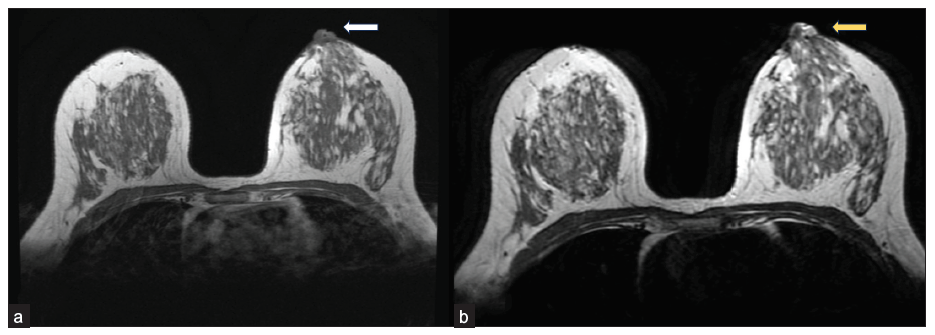
- On Magnetic Resonance Imaging (MRI), a circumscribed focal lesion of size 18 × 14 × 16 mm is seen within the left nipple, predominantly involving lateral half of the nipple. (a) shows intermediate signal intensity on T1WI (white arrow) and (b) shows heterogeneous hyperintensity (yellow arrow) on T2WI.
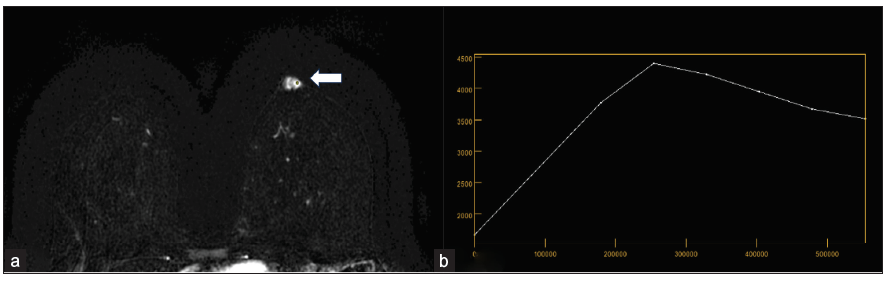
- On axial Magnetic Resonance Imaging (MRI) post contrast dynamic study, in (a) the lesion demonstrates intense enhancement (white arrow) and in (b) the lesion demonstrates type 2 kinetic curve.
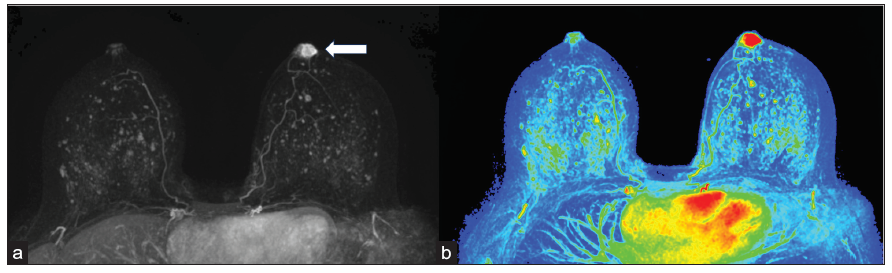
- (a) Axial maximum intensity projection (MIP) image of first post contrast Magnetic Resonance Imaging (MRI) subtraction shows asymmetric strong enhancement (white arrow) of the left nipple on grey scale and on (b) color coded maps.
A punch biopsy of the lesion was performed, which suggested a diagnosis of nipple adenoma. Considering the benign nature of the lesion and the absence of any suspicious features on imaging and histopathology, surgical excision was recommended for a definitive diagnosis and to alleviate the patient’s concern. A wide local excision of the nipple adenoma was performed under local anesthesia, followed by primary closure. The surgical specimen was sent for histopathological examination, which confirmed the initial diagnosis. Microscopy revealed an unencapsulated, fairly circumscribed area of adenosis comprising proliferating, small ducts in a sclerotic stroma. A few keratin cysts were also noted [Figure 5a]. A few of the duct lumina showed eosinophilic secretions [Figure 5b]. The ducts were lined by bland epithelial and myoepithelial cells. Extensive apocrine metaplasia was also noted [Figure 6]. The overlying stratified squamous epithelium of the nipple showed a focal area of erosion [Figure 5a]. These findings were consistent with the diagnosis of nipple adenoma.
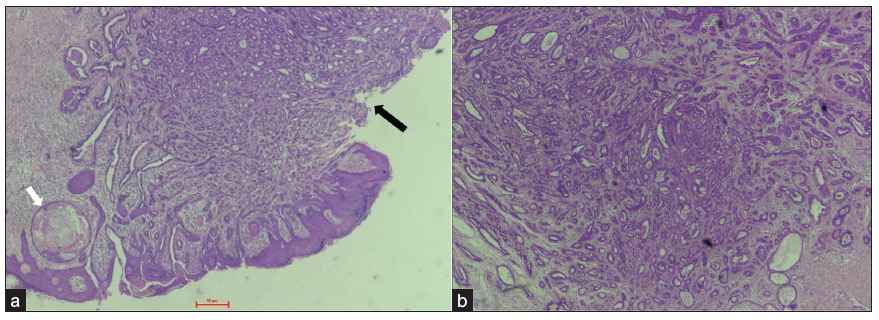
- (a) Photomicrograph of the left nipple biopsy showing focal erosion of the stratified squamous epithelium (black arrow). The underlying dermis shows an unencapsulated, circumscribed area of adenosis. A keratin cyst is also seen (white arrow). (H&E; 40x) (b) Benign proliferation of small ducts in a sclerotic stroma. Some of the duct lumina show eosinophilic secretions. (H&E; 40x). H&E: Hematoxylin and Eosin.
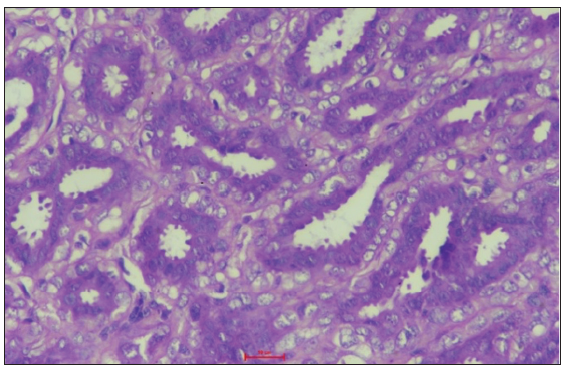
- The ducts are lined by cytologically bland epithelial and myoepithelial cells. Prominent apocrine change is seen in the epithelial cells. (H&E; 400x). H&E: Hematoxylin and Eosin.
DISCUSSION
Nipple adenoma is an unusual benign breast lesion that often poses a diagnostic challenge due to its rarity and overlapping clinical and radiological features with malignant neoplasms.
These are a rare benign pathology first described by Jones in 1955 as “florid papillomatosis of the nipple.”[2] The Japanese Breast Cancer Society has defined nipple adenoma as “a tumor developing papillary or solidly in the lactiferous duct of the nipple or just under the areola.”[3] It commonly affects women between the fourth and fifth decades of life.[2]
The lesion often presents clinically as a palpable or visible nodule in the nipple, which may have overlying erosion or discharge from associated ducts. In the presence of visible erosion through the skin of the nipple, nipple adenoma readily mimics a case of mammary Paget’s disease of the nipple or, even more rarely, squamous cell carcinoma of the nipple.[4] Both Nipple Adenoma and Paget disease can present with unilateral nipple enlargement, nipple nodules, skin changes including erosion, ulceration, or erythema, and/or sanguineous nipple discharge.[5] Clinically, nipple adenoma may also resemble eczema, psoriasis, or a skin infection.[6] Infection or inflammatory conditions have overlapping features but can be recognized due to distinct clinical presentation with erythema, edema, and skin thickening.[7]
Nipple adenoma has similar density as breast tissue; hence can be missed on conventional imaging modalities. Nipple adenoma is initially occult on mammography, but as it grows larger, it manifests as a well-defined, round, or oval mass localized within or beneath the nipple. Microcalcifications are typically absent. On ultrasonogram, they appear as hypoechoic or isoechoic hypervascular masses in the nipple, are typically circumscribed, and may have a lobulated appearance. However, these imaging features render it indistinguishable from a papilloma within the nipple on an ultrasonogram. On MRI, they appear as a well-defined, enhancing mass in the nipple region.[8] The extent of the tumor’s involvement is better assessed through MRI.[8] However, nipple adenoma may be confused with breast malignancy on MRI.[9] Histopathology and immunohistochemistry are required to establish the diagnosis.
Owing to the small size of the lesion, core needle biopsy is difficult to perform, and hence, punch or incisional biopsy remains the mainstay for preoperative diagnosis, followed by surgical excision for both definitive diagnosis and therapeutic purposes. Histopathology shows a fairly well-circumscribed but unencapsulated lesion with a florid epithelial proliferation of lactiferous ducts. Two distinct cell populations are present in these lesions: an exterior layer of myoepithelial cells and an inside layer of cuboidal epithelial cells with an apocrine secretion. The lesion may mimic ductal carcinoma on histology. However, the presence of a myoepithelial cell layer in neoplastic ducts, which can be confirmed by immunohistochemical stains like p63 and smooth muscle actin, differentiates adenoma from carcinoma.
If untreated, nipple adenomas may enlarge and cause local destruction.[10] These may be locally infiltrative, with the treatment of choice being surgical excision with clear margins. In our case, surgical excision with primary closure was performed. It is important to confirm diagnosis by histopathological analysis and confirm clear margins after tumor resection.
Early cases can be treated with minimally invasive techniques like Mohs micrographic surgery, nipple splitting enucleation, and cryotherapy, with better cosmetic restoration.[7] The prognosis is excellent, with low rates of recurrence after complete excision.
CONCLUSION
Nipple adenoma is a rare benign breast lesion of lactiferous ducts in the nipple region that can mimic the clinical presentation of more concerning breast malignancies. Awareness among clinicians, radiologists, and pathologists can help alleviate overtreatment and patient anxiety. Accurate histopathological diagnosis and subsequent surgical excision provide an excellent prognosis for patients. Further research and case studies are warranted to enhance our understanding of this uncommon breast lesion and its optimal management.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Nipple adenoma: A review of the literature. Ann Breast Surg. 2019;3:e8586.
- [CrossRef] [Google Scholar]
- Florid papillomatosis of the male nipple. Am J Surg. 2010;200:e39-e40.
- [CrossRef] [PubMed] [Google Scholar]
- Adenoma of the nipple: A clinicopathological report of 13 cases. Oncol Lett. 2014;7:1839-42.
- [CrossRef] [PubMed] [Google Scholar]
- Nipple adenoma: A benign disease with a suspicious presentation. The American SurgeonTM. 2022;0
- [Google Scholar]
- Diagnosis and surgical treatment of nipple adenoma. ANZ J Surg. 2015;85:444-7.
- [CrossRef] [PubMed] [Google Scholar]
- Nipple adenoma in a female patient presenting with persistent erythema of the right nipple skin: Case report, review of the literature, clinical implications, and relevancy to health care providers who evaluate and treat patients with dermatologic conditions of the breast skin. BMC Dermatol. 2016;16:4.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Nipple ultrasound: A pictorial essay. Korean J Radiol. 2020;21:955-66.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Adenoma of the nipple, focusing on the contrast-enhanced magnetic resonance imaging findings: Report of a case. Surg Today.. 2011;41:1138-41.
- [CrossRef] [PubMed] [Google Scholar]
- Adenoma of the nipple: A clinicopathological report of 13 cases. Oncol Lett. 2014;7:1839-42.
- [CrossRef] [PubMed] [Google Scholar]




