

Translate this page into:
Usefulness of intralesional contrast injection as a prebiopsy confirmation technique in a case of breast hemangioma

*Corresponding author: Priya Masilamani, Department of Radiology and Imaging Services, MGM Healthcare, Chennai, India. priya.ramprakash@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Masilamani P, Padala KP, Moorthy J, Subashchandrabose P. Usefulness of intralesional contrast injection as a prebiopsy confirmation technique in a case of breast hemangioma. Indian J Breast Imaging. 2024;2:39-43. doi: 10.25259/IJBI_22_2023
Abstract
Hemangiomas are uncommon benign vascular lesions of breast. They have nonspecific imaging features and can be isoechoic or hypoechoic or of heterogeneous echotexture in ultrasound (USG). When isoechoic, it may be difficult to identify these lesions with confidence against a fatty background. Here, we report such a case of a high-density lesion detected in screening mammogram, which was not so obvious in USG. We used the technique of intralesional contrast injection into the probable USG correlate for confirmation, before proceeding with the biopsy and establishing the diagnosis of hemangioma. Thus, this simple prebiopsy confirmation technique helps in identifying the definitive USG correlate, thereby facilitating a USG-guided biopsy. This is very useful, especially in the peripheral healthcare centers where stereotactic facility may not be available. Another learning point from this case is that in case of superficially located lesions that are readily visible in mammogram but less conspicuous in USG, the possibility of hemangioma can be considered in the differentials. This observation has been mentioned in other case reports as well and reiterated in our case. However, due to the nonspecific imaging features and low incidence, it is difficult to make diagnosis of hemangioma without tissue sampling. The imaging features of breast hemangioma in mammogram and ultrasound are reviewed and described in this case report with an emphasis on the role of intralesional contrast injection in lesion localization.
Keywords
Breast hemangioma
Intralesional contrast injection
Prebiopsy confirmation technique

INTRODUCTION
Breast hemangiomas are rare vascular malformations.[1] They are usually asymptomatic, nonpalpable masses detected in screening mammogram. The most common mammographic features described are oval or lobulated masses with well circumscribed or microlobulated margins. They are superficially located masses that appear hypoechoic or isoechoic or of heterogeneous echotexture in ultrasound (USG) with no internal vascularity. When these lesions are isoechoic in nature, identifying them in USG against the surrounding fat background may be challenging.[2] Probable USG correlates may be identified by carefully targeted USG in that particular quadrant focusing in the superficial plane and by using tissue hormonic imaging. In such cases, confirming the correlation between the lesion identified in mammogram and suspected lesion in USG should be done to avoid false negative biopsy. In this case, we performed a prebiopsy confirmation technique using USG-guided intralesional contrast injection followed by mammogram to ensure definitive correlation.
CASE REPORT
A 41-year-old female with no significant family history of breast cancer came for screening mammogram. Digital breast tomosynthesis was done in two standard imaging planes, namely craniocaudal and mediolateral oblique views using Hologic-Selenia dimensions mammography system. She had American College of Radiology (ACR) type B breast parenchyma (scattered fibro glandular tissue). Mammogram revealed an irregularly shaped high-density lesion (measuring 1.3 × 0.8cm) with microlobulated margins in the upper inner quadrant (UIQ) of the left breast [Figures 1 and 2]. There was no evidence of associated calcifications/architectural distortion/skin thickening/axillary lymphadenopathy. No other lesions were detected in the breast.
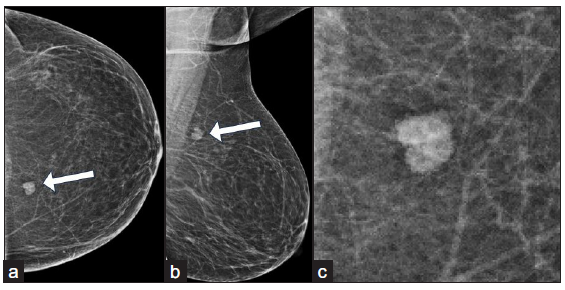
- (a-b) Screening mammogram of a 41-year-old woman—Craniocaudal and mediolateral oblique views shows an irregularly shaped high density lesion (white arrows) with microlobulated margins in the upper inner quadrant of left breast. There is no evidence of associated calcifications/architectural distortion-associated features. (c) Magnified image of the same lesion in Craniocaudal view of left breast depicts the microlobulated margins.
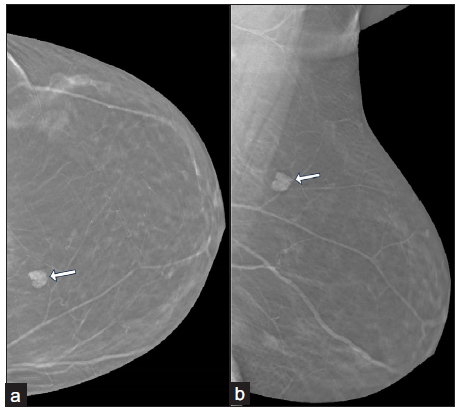
- (a-b) Tomosynthesis images of left breast in craniocaudal and mediolateral oblique views show an irregularly shaped high density lesion (white arrows) with microlobulated margins in the upper inner quadrant. The tomosynthesis slice number (43/62 in craniocaudal view and 55/72 in mediolateral oblique view) denotes the superficial location of the lesion.
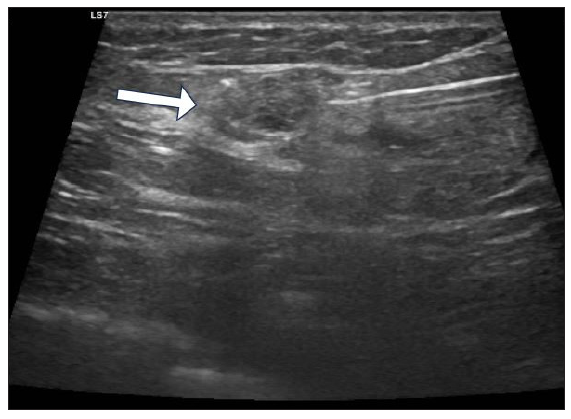
The patient underwent USG with high frequency transducer (GE Logiq S7) to further characterize the lesion. There was no palpable abnormality, and on the initial USG, it was surprising to note that a lesion so evident in mammogram could not be identified in USG. Review of tomosynthesis images showed the superficial location of the lesion in UIQ. On targeted review of USG in the UIQ in the subcutaneous fat plane using tissue hormonic imaging, a probable USG correlate was identified—an irregular shaped, subtle iso to mildly hyperechoic lesion (measuring 1.2 × 0.6 cm) in parallel orientation with no posterior features or internal vascularity at 10 o’clock position circle 3 zone A [Figure 3]. The lesion was assigned a BIRADS-4A category due to the presence of microlobulations, and an image-guided biopsy from the same was recommended. A lesion is usually sampled under the guidance of the modality in which it is best visualized, which was mammogram in our case. But, since we did not have provision for stereotactic biopsy, we decided to sample the lesion under USG guidance after ensuring concordance of the USG correlate with the mammogram detected lesion. So we injected 1–2 cc of diluted contrast agent (0.5 cc of nonionic iodine-based contrast agent diluted with 5 cc of distilled water) percutaneously under aseptic precautions into the suspected lesion using 24G needle under USG guidance. Immediately after, the mammogram of left breast was taken in craniocaudal and mediolateral oblique views which showed the presence of streaks of radio opaque contrast within and around the lesion, thereby establishing concordance [Figure 4]. We confidently proceeded with a USG-guided biopsy of the lesion using 14G biopsy needle, obtaining three cores [Figure 5]. The histopathological examination revealed ectatic dilated vascular spaces of varying shapes and sizes lined by flat to cuboidal epithelium [Figures 6–8] consistent with a hemangioma.
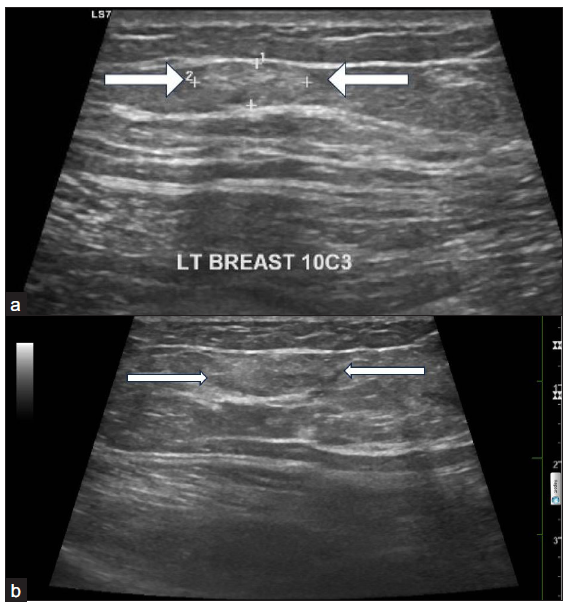
- (a-b) Grey scale USG images reveals an irregularly shaped, subtle iso to mildly hyperechoic lesion with microlobulations in parallel orientation in the superficial plane (white arrows). USG: ultrasound.
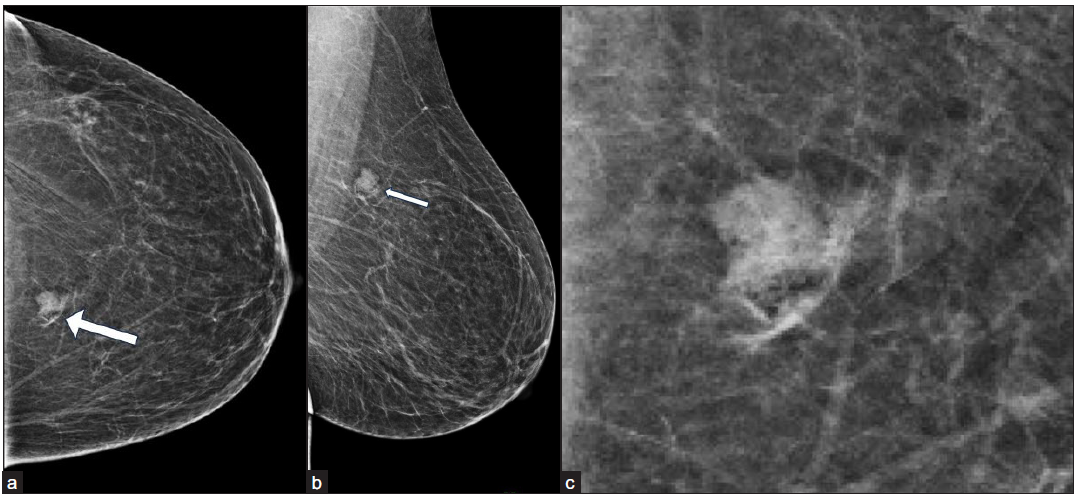
- (a-b) Left breast mammogram—craniocaudal and mediolateral oblique views—after intralesional injection of contrast shows streaks of contrast in and around the lesion (white arrow). (c) Magnified image of the same lesion in left breast mammogram—craniocaudal view—after intralesional injection of contrast shows streaks of contrast in and around the lesion.
- USG-guided core biopsy of the lesion (white arrow). USG: ultrasound.

- Multiple linear cores showing a neoplasm composed of large, dilated, thin-walled blood vessels (Hematoxylin and Eosin stain 4x).
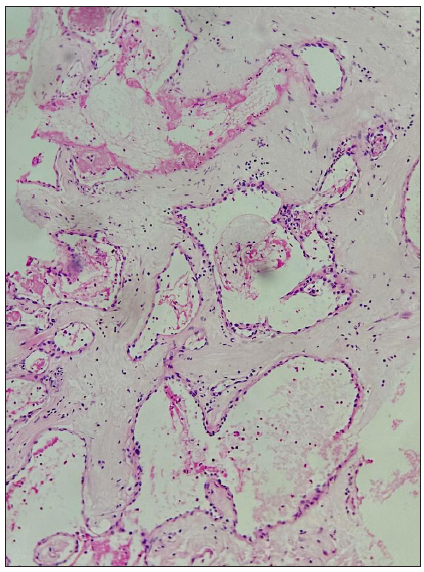
- Large, dilated, congested, thin-walled blood vessels lined by flat endothelium (Hematoxylin and Eosin stain 10x).
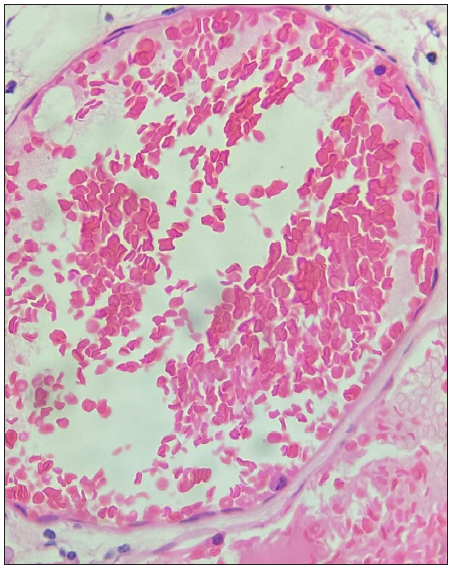
- High power view showing congestion and flat endothelial lining cells (Hematoxylin and Eosin stain 40x).
Retrospectively analyzing a superficially located high density lesion on mammogram with an isoechoic appearance in USG was concordant with the diagnosis of hemangioma. Since it was a case of hemangioma with no evidence of atypia, the patient was advised to come for follow-up USG after six months.
DISCUSSION
Hemangiomas are rare benign tumors of vascular origin, with the other vascular tumors being angiolipomas and angiosarcomas. Breast hemangiomas are found in 1.2% of mastectomy specimens and 11% of postmortem specimens of female breast.[3] They occur in adult women over a wide age range. Depending on the size of the vessels involved, hemangiomas are classified into two common types—capillary and cavernous.
Most hemangiomas in breast are extra parenchymal and are located superficially in subcutaneous fat.[4] The common imaging features of hemangiomas are oval or lobulated masses with well-circumscribed or microlobulated margins and a non-hyperechoic echotexture (hypoechoic/isoechoic/heterogeneous). Though vascular in nature, hypovascularity has been reported in hemangiomas. However, the findings are nonspecific, which rendered the low incidence of diagnosis of breast hemangiomas. Rarely the mammogram may show characteristic phleboliths.
Hemangiomas, despite being readily visible in mammogram, may be difficult to identify sonographically because of their isoechoic or slightly hypoechoic appearance against a fatty background.[5] In such cases, adequate positioning of the focus in superficial plane with tissue hormonic imaging may increase the visibility of the lesion in USG.[5] When the lesion is still not visible in USG in spite of a careful search, stereotactic-guided biopsy is done. In cases where there is a suspected USG correlate, intralesional contrast injection can be done before proceeding with a USG-guided biopsy. This step is essential to ensure that we are targeting the correct lesion, thus avoiding false negative biopsy. Such tailored techniques become all the more important in centers where provision for biopsy under stereotactic guidance is not available.
Yasemin Kayadibi et al. described a prebiopsy confirmation technique, which uses an ultrasound-guided intralesional contrast injection followed by a nonenhanced magnetic resonance imaging (MRI) sequence to identify sonographic correlations with incidentally detected MRI lesions.[6] Such prebiopsy lesion marking methods are important to ensure definite correlation.
Breast hemangiomas can be managed conservatively or with surgical excision. Earlier hemangiomas were surgically excised to rule out any angiosarcoma component. But since malignant transformation is extremely rare, asymptomatic hemangiomas with classic imaging features, radio pathologic concordance, and no atypia on biopsy can be managed conservatively with follow-up imaging.[7] Features such as size larger than 2 cm, irregular shape, hypervascularity in Doppler imaging, and invasive growth pattern are more common with angiosarcoma and may warrant surgical excision.[8] Intraparenchymal location of the lesion is also common with angiosarcomas, and these show atypical proliferating blood vessels with nuclear atypia and increased mitotic activity. While endothelial markers such as CD 31 and CD 34 denote the vascular nature of the lesion, a lower Ki-67 proliferation rate can be used to differentiate hemangiomas from angiosarcoma in case of diagnostic dilemmas.[9]
CONCLUSION
Breast hemangiomas are rare vascular tumors which lack specific imaging features. However, hemangioma can be considered as differential when oval or lobulated superficial lesions are detected in mammogram with less obvious USG correlates. Intralesional contrast injection is a simple, safe, and useful prebiopsy confirmation technique to confidently identify sonographic correlates in such cases, thus facilitating USG-guided biopsy for tissue diagnosis.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Breast hemangioma evaluation with magnetic resonance imaging: A rare case report. Eur J Breast Health. 2022;18:190-4.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Vascular tumors of the breast: Mammographic, sonographic, and MRI appearances. AJR Am J Roentgenol. 2005;184:331-8.
- [CrossRef] [PubMed] [Google Scholar]
- Incidence of perilobular hemangioma in the female breast. Arch Pathol Lab Med. 1983;107:308-10.
- [PubMed] [Google Scholar]
- The blue alert: An unusual case report of breast hemangioma. Egypt J Radiol Nucl Med. 2022;53:221.
- [CrossRef] [Google Scholar]
- Sonographic and mammographic appearances of breast hemangioma. AJR Am J Roentgenol. 2008;191:W17-22.
- [CrossRef] [PubMed] [Google Scholar]
- Second look ultrasonography-guided breast biopsy with magnetic resonance imaging confirmation by intralesional contrast injection. Eur J Breast Health. 2020;17:1-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Vascular abnormalities of the breast: Arterial and venous disorders, vascular masses, and mimic lesions with radiologic-pathologic correlation. Radiographics. 2011;31:E117-36.
- [CrossRef] [PubMed] [Google Scholar]
- Breast hemangiomas: Imaging features with histopathology correlation. J Breast Imaging. 2024;6:288-95.
- [CrossRef] [PubMed] [Google Scholar]
- Hemangiomas and angiosarcomas of the breast: Diagnostic utility of cell cycle markers with emphasis on Ki-67. Arch Pathol Lab Med. 2007;131:538-44.
- [CrossRef] [PubMed] [Google Scholar]




