

Translate this page into:
Diffusion weighted imaging as adjunct modality to distinguish benign and malignant breast lesions in resource constrained settings: A single institute experience

*Corresponding author: Varsha Kaginalkar, Department of Radiodiagnosis, GMC Chh. Sambhajinagar, (Aurangabad), Maharashtra, India. kaginalkar@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kaginalkar V, Arora N, Shukla A. Diffusion weighted imaging as adjunct modality to distinguish benign and malignant breast lesions in resource constrained settings: A single institute experience. Indian J Breast Imaging. 2024;2(2):83–90. doi: 10.25259/IJBI_23_2024
Abstract
Objectives
To establish the accuracy of the “targeted DWI/ADC sequence” as an adjunct to mammography and sonography for differentiating malignant and benign breast masses in an underdeveloped population, in correlation with histopathology.
Materials and Methods
The study population was predominantly rural and from underdeveloped regions. It included 108 female patients of various ages who presented with breast masses with equivocal diagnoses on mammography and sonography. These patients were unwilling to return for additional investigations. The targeted lesions were then further evaluated using diffusion weighted imaging (DWI)/apparent diffusion coefficient (ADC) maps and ADC values. The final diagnosis was later confirmed by histopathology examination.
Results
A total of 108 patients having 115 lesions were targeted based on mammography and sonography findings and subjected to DWI. The cut-off ADC value was established for these lesions to be 1.2 × 10–3 mm2/s through receiver operating characteristic curve analysis. This value exhibited a sensitivity of 98.7% and specificity of 91.9% in the present study. DWI overdiagnosed malignancy by 2.6%.
Conclusion
In the present study, the “targeted DWI/ADC sequence” has proven useful with a sensitivity of 98.7% and specificity of 91.9% using a cut-off value of 1.2 × 10–3 mm2/s. Targeted DWI/ADC in combination with mammography and sonography accurately identified all malignant lesions with overdiagnosis of malignancy in 2.6% of cases. In India, where the demographic is largely rural and underdeveloped, social and economic limitations, along with a lack of awareness, make adherence to ideal diagnostic protocols challenging. This ultimately results in losing the patient to follow-up and missing the cancer. This novel approach of targeted DWI/ADC sequence in combination with mammography and sonography is highly effective in such scenarios, enabling the identification of the likely nature of the disease during the same visit. This empowered healthcare professionals to counsel patients confidently and initiate early management.
Keywords
ADC threshold value
DWI/ADC
Low resource settings
Malignant breast lesions
MRI

INTRODUCTION
Diagnosing breast malignancy in low-resource settings, especially in low- and middle-income countries, remains a challenge when mammography and sonography yield inconclusive results. For many women, an ideal multimodality diagnostic approach is often unattainable due to the burden of repeated visits adding to financial and family constraints, resulting in delayed or missed diagnoses.
As clinical radiologists, we need to take into consideration these social constraints, thus approaching each case in a patient-centric manner.
With this background, we planned to introduce a “targeted Diffusion Weighted Imaging (DWI) sequence” as a cost-effective, rapid adjunct in the workup of equivocal findings seen on conventional imaging modalities for distinguishing malignant from benign lesions, facilitating same-visit diagnosis.
Breast cancer is the most common cancer in women worldwide.[1,2] Despite advances in imaging, distinguishing benign from malignant lesions often requires further imaging or invasive tests, highlighting the need for quick, precise, non-invasive diagnostics.
DWI, introduced by Stejskal and Tanner in 1965,[3] measures the motion of water molecules in tissues, which depends on their composition. With the obtained DWI, diffusion constant maps called the ADC maps are generated, which quantify the diffusion in tissues and can be used to study the abnormalities in tissue structures. DWI has high sensitivity and specificity in distinguishing malignant and benign breast lesions.[4,5]
We planned to supplement equivocal cases on mammography and sonography by using a basic non-contrast sequence (T1 and T2 weighted axial) and one functional imaging DWI.
MATERIALS AND METHODS
This study aims to establish the accuracy of the “targeted DWI/ ADC sequence” as an adjunct to mammography and sonography for differentiating malignant and benign breast masses.
Study Design
This was a prospective observational diagnostic study involving female patients with palpable breast masses. The study employed mammography, sonography, and DWI imaging. All patients underwent histopathological correlation, and the study received institutional review board approval.
Inclusion Criteria
The study included female patients of all ages with a history of palpable breast masses with equivocal diagnoses on mammography and sonography who provided informed consent.
Exclusion Criteria
Excluded were patients unwilling to participate, those with Magnetic resonance imaging (MRI) contraindications (e.g., metallic implants and claustrophobia).
Equipment Used
The study utilized a GE Signa 3.0T MRI machine equipped with a dedicated phased-array bilateral breast coil.
Patient Preparation
The patient is checked as per MRI safety protocol before the scan like: Patients removed metallic belongings and were positioned in the prone position with their arms extended above their heads. The breasts were secured to minimize motion artifacts. Patients were explained about the examination and the scan time.
Protocol
The imaging protocol included basic non-contrast sequences—T1 and T2-weighted axial and one functional imaging—diffusion-weighted single-shot spin echo echoplanar imaging sequence (SS SE EPI) [Table 1].[6,7]
| Sequence | TR/TE (msec) | Slice thickness/gap (mm) | FOV (cm) | Matrix |
| T1 TSE | 537/10 | 3/3 | 25–41.7 | 168 × 222 |
| T2 TSE | 388/12 | 3/3 | 25–41.2 | 216 × 264 |
| T2 SPAIR | 488/12 | 3/3 | 25–41.2 | 160 × 207 |
| T2 COR | 388/12 | 3/3 | 30–41.1 | 260 × 264 |
| DWI | 5754/97 | 5/0 | 27–40 | 332 × 133 |
TR: Repetition time, TE: Echo time, DWI: Diffusion weighted imaging, TSE: Turbo spin echo, SPAIR: Spectral attenuated inversion recovery, COR: Coronal, FOV: Field of view, MRI: Magnetic resonance imaging.
Image Analysis
Lesions were found, evaluated, and targeted based on mammography and sonography and then characterized on above-mentioned MRI sequences[8,9] by a senior radiologist. All lesions, irrespective of their size, were included in the analysis. DWI with a high b value was used in this study, as ADC values are strongly affected by perfusion in the case of small b values.[10,11] Accordingly, this study was performed using b 0, 800, and 1000 values. The ADC values were calculated on the workstation by applying the region of interest (ROI) on the lesions in the ADC maps determined for each patient.
The ADC value of the normal breast parenchyma was also calculated on the workstation in every patient by applying ROI in the region of the breast with no obvious lesion or in the contralateral breast if lesion-free. Small lesions of size 1–2 cm seen in the vicinity of a large mass, showing similar signal intensity as the main lesion, were called as satellite lesions in the study. These lesions were only assessed for their presence or absence and not for ADC value.
The area under the receiver operating characteristic curve (ROC) was used for plotting ADC cut-off values. Since MRI is inherently a sensitive investigation, the cut-off value with high specificity of 95% was chosen in this study.
Diagnosis Confirmation
Diagnosis was confirmed on the histopathological study of post-surgical or ultrasound guided core needle biopsied samples.
RESULTS
-
108 female patients with 115 lesions were assessed in our study with the distribution of benign and malignant lesions according to HP and DWI findings [Table 2].
Table 2: Distribution of lesions according to HP and DWI findings.ADC coefficient HP report Benign 39 42 Malignant 76 73 Total 115 115 HP: Histopathology, DWI: Diffusion weighted imaging, ADC: Apparent diffusion coefficient.
Mean ADC value of normal breast parenchyma in our study was 2.07 ± 0.079 × 10–3 mm2/s.
-
The cut-off ADC value determined in this study was 1.2 × 10–3 mm2/s, having a sensitivity of 98.7% and specificity of 91.9% by ROC analysis [Figure 1].
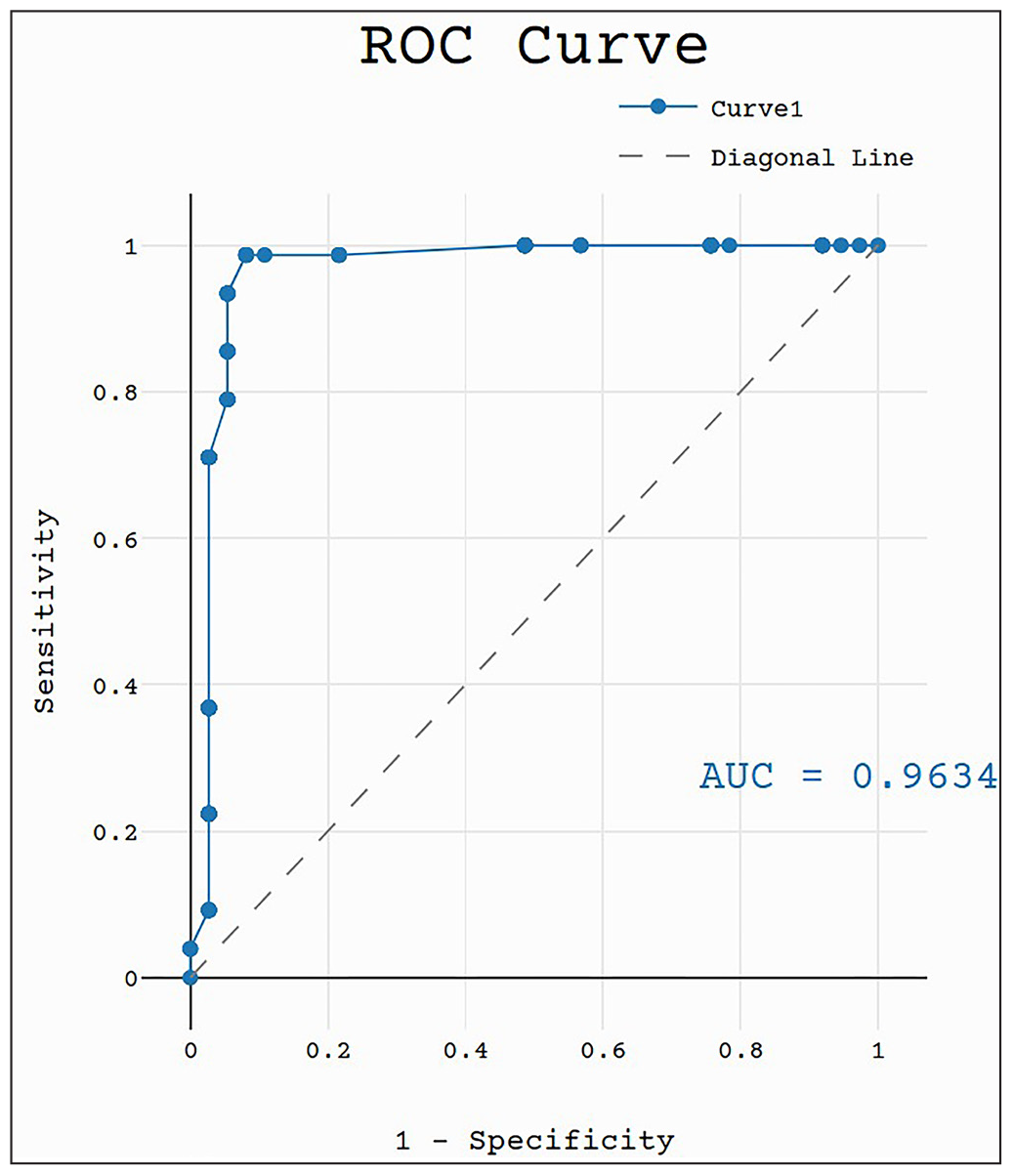 Figure 1:
Figure 1:- Receiver operating characteristic (ROC) curve analysis to calculate apparent diffusion coefficient cut-off value. AUC: Area under curve.
-
ADC value correlation of malignant lesions with their histopathological reports [Table 3].
Table 3: Distribution of malignant lesions with their DWI, ADC features, and ADC values.Type of lesion on histopathology Number of lesions DWI at B 1,000 ADC on map Mean ADC value ( × 10–3 mm2/s) Invasive ductal carcinoma 49 ↑ ↓ 0.98 ± 0.04 Ductal carcinoma 20 ↑ ↓ 1.12 ± 0.06 Lobular carcinoma 5 ↑ ↓ 0.82 Inflammatory breast carcinoma 1 ↑ ↓ 0.87 Malignant transformation of phyllodes 1 ↑ ↓ 0.4 ↑: High signal intensity, ↓: Low signal intensity, DWI: Diffusion weighted imaging, ADC: Apparent diffusion coefficient.
Mean ADC value of malignant lesion: 0.95 ± 0.02 × 10–3 mm2/s.
All malignant lesions in the study were identified correctly, demonstrating high signal intensity on DWI and low signal intensity on the ADC map with ADC values below the calculated cut-off.
-
ADC value correlation of benign lesions with their histopathological reports has been tabulated in Table 4.
Table 4: Distribution of benign lesions with their DWI, ADC features, and ADC values.Type of lesion on histopathology Number of lesions DWI at B 1,000 ADC on map Mean ADC value (× 10–3 mm2/s) Fibroadenomas 12 ↑ ↓ 1.5 × 10–3 ± 0.014 Intraductal papilloma 7 ↑ ↓ 1.39 ± 0.08 Breast abscess 2 ↑ ↓ 1.38 Lymph nodes 5 ↑ ↓ 1.18 Postoperative lesions 7 ↑ ↓ 1.878 Phyllodes 4 ↑ ↓ 1.42 Fibrocystic disease 2 ↑ ↓ 1.9 ↑: High signal intensity, ↓: Low signal intensity, DWI: Diffusion weighted imaging, ADC: Apparent diffusion coefficient.
Mean ADC value of benign lesion: 1.51 ± 0.09 × 10–3 mm2/s.
All benign lesions in the study demonstrated high signal intensity on DWI and ADC except cellular fibroadenoma, fibroadenosis, and one abscess, having ADC values below the cut-off calculated.
Two patients were diagnosed with abscesses; one showed ADC value above the cut-off and one showed ADC value below the cut-off.
DISCUSSION
Our department majorly caters to a rural, underdeveloped demographic where people have a lot of social stigma, fear, and negligence about breast diseases. This situation compels the breast radiologist to arrive at the closest differential diagnosis at the same sitting when the patient comes for the first evaluation.
In this study, “targeted DWI/ADC sequence” is used as an additional tool in cases where sonography and mammography are equivocal, and patients were unwilling to undergo any further investigation, including biopsy or revisit for the same.
DWI/ADC sequence is cost-effective, quick, and non-invasive, which are essential factors for acceptance by the patient while supplementing conventional investigations.
A total of 108 patients with 115 breast lesions were evaluated using mammography, sonography, and DWI. Through ROC analysis, a cut-off ADC value of 1.2 × 10–3 mm2/s was established, demonstrating a sensitivity of 98.7% and specificity of 91.9%. Among the 115 lesions, 76 showed diffusion restriction with ADC values below the cut-off. Of these, 73 were confirmed as malignant on histopathology (true positives), while three were false positives. Notably, no false negatives were identified in this study, and DWI overdiagnosed malignancy by only 2.6%, highlighting its reliability in the lesion assessment.
The sensitivity and specificity of DWI was comparable with studies by Chen et al. [11] and Yadav et al. [12] [Table 5].
All malignant lesions in the study demonstrated high signal intensity on DWI and low signal intensity on ADC map with ADC values below the calculated cut-off [Figure 2].

- Inflammatory breast carcinoma: A 49-year-old female with inflammatory breast carcinoma in left breast appears; (a) hypointense on T1W, (b) heterogeneous on T2W image, (c) hyperintense on T2W Spectral attenuated inversion recovery. (d-e) Diffusion weighted imaging (DWI) at b value = 0 shows hyperintensity. (f) Apparent diffusion coefficient map shows hypointensity.
In this study, all benign lesions [Figure 3] exhibited high signal intensity on DWI and ADC, with ADC values above the calculated cut-off, except for cellular (juvenile) fibroadenoma[13] [Figure 4], fibroadenosis, and one abscess. These exceptions had ADC values of 0.91 × 10–3 mm2/s, 1.02 × 10–3 mm2/s, and 0.4 × 10–3 mm2/s, respectively, falling below the benign threshold.

- Typical Fibroadenoma: A 48-year-old female with mass in left breast: (a) T1W image shows a circumscribed hypointense mass in left breast. (b and c) T2W and T2W Spectral attenuated inversion recovery (SPAIR) images show hyperintense mass. (d and e) Diffusion weighted imaging with b value = 0 and 1,000 shows hyperintensity. (f) Apparent diffusion coefficient map shows hyperintensity.

- Cellular (juvenile) fibroadenoma: A 15-year-old female with cellular (juvenile) fibroadenoma: (a) T1W image shows a circumscribed hypointense mass in the left subaerolar region. (b and c) T2W and T2W Spectral attenuated inversion recovery images show hyperintense mass. (d and e) Diffusion weighted imaging at b value = 0 shows hyperintensity, and at b value = 1,000 shows hypointensity. (f) Apparent diffusion coefficient (ADC) map shows hypointensity (ADC value = 0.71 × 10–3 mm2/s). This could be secondary to the high cellularity of the lesion.
This false-positive result is likely due to the longer T2 relaxation time of these lesions.[13] Juvenile fibroadenoma, as defined by Stanford Medical School, is characterized by hypercellular stroma, contributing to restricted diffusion and low ADC values.[14,15] Similarly, densely packed cells in fibroadenosis restrict water molecule movement, mimicking malignant lesions. Parsian S. et al.[15] corroborate these findings, linking low ADC values in such cases to increased cellularity and dense collagenous stroma. In abscesses, ADC values vary depending on the stage of infection and treatment, potentially falling above or below the cut-off [16] [Figure 5].

- Breast abscess: A 28-year-old female with lump and pain in right breast since 10 days: (a) Hypointense on T1, (b) Heterointense on T2, (c) Diffusion weighted imaging at b value = 800 shows diffusion restriction, and (d) Apparent diffusion coefficient map shows hypointensity.
To address these diagnostic challenges, it is essential to consider the morphological characteristics[17,18] of the lesions and recommend a core needle biopsy when necessary.
In this study, the mean ADC values[19] were:
Normal breast parenchyma: 2.07 ± 0.079 × 10–3 mm2/s
Benign lesions: 1.51 ± 0.09 × 10–3 mm2/s
Malignant lesions: 0.95 ± 0.02 × 10–3 mm2/s
Comparison of ADC threshold values for differentiating malignant from benign lesions and their sensitivities and specificities with some of the other studies has been tabulated in Table 6.[20–22]
| Study | ADC Threshold value | Sensitivity | Specificity |
| Marini et al.[9] | 1.1 | 80.0 | 81.0 |
| Guo et al.[17] | 1.3 | 93.0 | 88.0 |
| Woodhams et al.[21] | 1.6 | 93.0 | 46.0 |
| Rubesova et al.[22] | 1.13 | 86.0 | 86.0 |
| Luoet et al.[18] | 1.22 | 88.9 | 87.9 |
| Pereira et al.[5] | 1.2 | 92.3 | 96.2 |
| Palle L. et al.[20] | 1.3–1.5 for benign diseases 0.8–1.1 for malignant diseases | 97.2 | 100 |
| Orguc et al.[19] | 1.23 | 82.8 | 90.0 |
| Present study | 1.2 | 98.7 | 91.9 |
ADC: Apparent diffusion coefficient.
Importantly, DWI/ADC correctly identified all eight lesions of approximately 1 cm in size, of which seven were benign and one was malignant. These findings emphasize the potential of DWI/ADC as a reliable diagnostic tool.
Limitations
DWI is known to be susceptible to various image quality artifacts;[23] all images in this study were interpretable, without T2 shine-through or T2 black-out artifacts. DWI, however, remains sensitive to motion, and patient cooperation during the scan.
Although the negative predictive value of DWI for lesions smaller than 1 cm is typically considered low,[22] this study successfully interpreted all small lesions.
DWI and ADC are invaluable tools; however, they have limitations in specificity which underscore the importance of combining them with other imaging modalities, viz., mammography and ultrasonography, for a comprehensive diagnosis.
CONCLUSION
In the present study, the “targeted DWI/ADC sequence” has proven useful with sensitivity of 98.7% and a specificity of 91.9% using a cut-off value of 1.2 × 10–3 mm2/s. Targeted DWI/ADC in combination with mammography and sonography accurately identified all malignant lesions with overdiagnosis of malignancy in 2.6% of cases. In India, where the demographic is largely rural and underdeveloped, social and economic limitations, along with a lack of awareness, make adherence to ideal diagnostic protocols challenging. This ultimately results in losing the patient to follow-up and missing the cancer.
This approach of targeted DWI/ADC sequence in combination with mammography and sonography can be highly effective in such scenarios, enabling the identification of the likely nature of the disease during the same visit. This empowered healthcare professionals to counsel patients confidently and initiate early management.
Ethical approval
The research/study approved by the Ethics Committees of the Government Medical College, Aurangabad, Maharashtra, number Pharma/IEC-GMCA/460/2017, dated 23th October 2017.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Breast cancer statistics 2024. CA Cancer J Clin.. 2024;74((6)):477-495.
- [CrossRef] [PubMed] [Google Scholar]
- Meta-analysis of quantitative diffusion-weighted MR imaging in the differential diagnosis of breast lesions. BMC Cancer.. 2010;10:693.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Diffusion MRI outside the brain: a case-based review and clinical applications. 2012:400p.
- [Google Scholar]
- Contribution of diffusion-weighted imaging to dynamic contrast-enhanced MRI in the characterization of breast tumors. AJR Am J Roentgenol.. 2011;196((1)):210-7.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment of breast lesions with diffusion-weighted MRI: comparing the use of different b values. AJR Am J Roentgenol.. 2009;193:1030-5. [published correction appears in AJR Am J Roentgenol. 2011;196:477].
- [CrossRef] [PubMed] [Google Scholar]
- Diagnostic assessment by dynamic contrast-enhanced and diffusion-weighted magnetic resonance in differentiation of breast lesions under different imaging protocols. BMC Cancer.. 2014;14:366.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Apparent diffusion coefficient as an MR imaging biomarker of low-risk ductal carcinoma in situ: a pilot study. Radiology.. 2011;260:364-72.
- [CrossRef] [PubMed] [Google Scholar]
- Contrast-enhanced magnetic resonance mammography: Does it affect surgical decision-making in patients with breast cancer? Breast Cancer Res Treat.. 2007;106:65-74.
- [Google Scholar]
- Quantitative diffusion-weighted MR imaging in the differential diagnosis of breast lesion. Eur Radiol.. 2007;17:2646-55.
- [CrossRef] [PubMed] [Google Scholar]
- Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology.. 1988;168:497-505.
- [CrossRef] [PubMed] [Google Scholar]
- Conspicuity of breast lesions at different b values on diffusion-weighted imaging. BMC Cancer.. 2012;12:334.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Effectivity of combined diffusion-weighted imaging and contrast-enhanced MRI in malignant and benign breast lesions. Pol J Radiol.. 2018;83:e82-e93.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Role of quantitative analysis of T2 relaxation time in differentiating benign from malignant breast lesions. J Int Med Res.. 2018;46:1928-35.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Juvenile fibroadenoma of the breast. Stanford School of Medicine. http://surgpathcriteria.stanford.edu/breast/juvfibroadenoma/.
- [Google Scholar]
- Diffusion-weighted imaging reflects variable cellularity and stromal density present in breast fibroadenomas. Clin Imaging.. 2016;40:1047-54.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Diffusion-weighted imaging in the assessment of brain abscesses therapy. AJNR Am J Neuroradiol.. 2004;25:1310-7.
- [PubMed] [PubMed Central] [Google Scholar]
- Differentiation of clinically benign and malignant breast lesions using diffusion-weighted imaging. J Magn Reson Imaging.. 2002;16:172-8.
- [CrossRef] [PubMed] [Google Scholar]
- Application of diffusion weighted magnetic resonance imaging to differential diagnosis of breast diseases. Chin J Cancer.. 2007;26:168-71.
- [PubMed] [Google Scholar]
- Diffusion-weighted MR imaging of the breast: comparison of apparent diffusion coefficient values of normal breast tissue with benign and malignant breast lesions. Singapore Med J.. 2012;53((11)):737-43.
- [PubMed] [Google Scholar]
- Role of diffusion MRI in characterizing benign and malignant breast lesions. Indian J Radiol Imaging.. 2009;19:287-90.
- [Google Scholar]
- Diffusion-weighted imaging of malignant breast tumors: The usefulness of apparent diffusion coefficient (ADC) value and ADC map for the detection of malignant breast tumors and evaluation of cancer extension. J Comput Assist Tomogr.. 2005;29((5)):644-9.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative diffusion imaging in breast cancer: A clinical prospective study. J Magn Reson Imaging.. 2006;24:319-24.
- [CrossRef] [PubMed] [Google Scholar]
- Diffusion-weighted magnetic resonance imaging for breast cancer screening in high-risk women: design and imaging protocol of a prospective multicenter study in Korea. J Breast Cancer.. 2021;24:218-28. [published correction appears in J Breast Cancer. 2022;25:145–6.].
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




