

Translate this page into:
Imaging in Paget disease of breast

*Corresponding author: Pratiksha Yadav, Department of Radiology and Interventional Radiology, Dr. D. Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, Maharashtra, India. yadavpratiksha@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Yadav P, Koppal D. Imaging in Paget disease of breast. Indian J Breast Imaging. 2025;3:39–46. doi: 10.25259/IJBI_27_2024
Abstract
Paget disease is a rare malignancy that involves the nipple and areola and infiltrates the skin of the nipple by adenocarcinoma. It is essential to diagnose it correctly, as more than 90% of Paget disease cases are associated with underlying breast cancer. It is usually associated with ductal carcinoma in situ (DCIS) involving the lactiferous ducts at the nipple-areolar complex. However, it may be associated with DCIS or invasive breast carcinoma in the breast parenchyma at distant locations. Mammography may not detect Paget disease in approximately 50% of cases. A multimodality imaging approach is suggested to evaluate the nipple-areolar complex and underlying breast with breast ultrasound and dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) in negative mammograms. Radiology investigations are helpful in appropriate surgical treatment and monitoring. This article describes the spectrum of imaging findings on various radiology modalities and characteristic clinical and pathological features of Paget’s disease.
Keywords
Breast cancer
DCIS
Invasive cancer
Nipple areolar
Paget

INTRODUCTION
Paget disease is a rare type of cancer of the nipple and areola, and it was first explained by a British doctor, Sir James Paget, in 1874.[1] He studied the relationship between changes in the skin of the nipple-areolar region and breast cancer.[1] It is characterized clinically by nipple erythema and irritation along with pruritus that may progress to form a crust and ulcer on the affected nipple. The condition may spread from the nipple and involve the areola and surrounding breast skin. The differential diagnosis of erythematic, itchy, and scaly skin of the nipple-areola complex includes eczema, contact dermatitis, and Paget disease. Paget disease causes infiltration of the epidermis of the nipple and areola by the adenomatous cells, which appear as round cells under the microscope with an increased nucleus-to-cytoplasmic ratio. Prevalence of an associated breast cancer may be observed in 67–100% in some studies.[1] Ninety percent of the cases may be associated with other coexisting occult breast cancers such as ductal carcinoma in situ (DCIS) and invasive ductal carcinoma.[2–4] Paget cells in biopsy from skin confirms the diagnosis and role of imaging is primarily to ascertain presence of any underlying breast cancer. Imaging also helps surgeons make decisions regarding appropriate management. The necessary modalities used for breast imaging in such cases are mammography, ultrasound, and magnetic resonance imaging (MRI) of both breasts. We discuss the clinical features, histopathology findings, and differential diagnosis and demonstrate the imaging findings of Paget disease on mammography, ultrasound, and MRI. Management and the role of imaging in treatment planning have also been discussed.
EPIDEMIOLOGY
Although Paget disease can be encountered in both genders; it is more commonly seen in females with mean age of 57 years. Approximately 1–4% of all cases of breast cancer are also associated with Paget disease of the same breast.[2,3] Patients usually complain of itching, redness, or tingling in the nipple-areolar region. There can be associated nipple discharge, flaky, crusty and thickened nipple and areola. Nipple morphology may be altered either as a flat or inverted nipple. All these symptoms of Paget disease are similar to other dermatological conditions such as eczema or dermatitis.[1–3] Many times, this similarity leads to the delayed diagnosis of Paget’s disease. Hence, the clinician should be aware and cautious regarding these features of the nipple-areola complex and evaluate the condition thoroughly to rule out the presence of associated breast cancer. Patients with Paget disease may present with a palpable mass in the breast. It has been documented that patients with no associated palpable lump have a better prognosis than the ones with a mass.[5]
Paget Disease and Breast Carcinoma
Many patients of Paget disease will not have mammographic findings at the time of diagnosis.
There has been association with breast carcinoma, either DCIS, invasive breast carcinoma, or both.
The associated breast carcinoma can be seen either in the nipple or, in the vicinity of the nipple-areolar complex (NAC) or elsewhere in the same breast.[6]
PATHOGENESIS
Hypothesis for the Concordance of Paget Disease and Breast Malignancy
Two essential and acceptable hypotheses have been proposed associating the correlation.
The epidermotropic theory: the Paget cells represent the carcinomatous spread of the breast malignancy through the retroareolar ducts to the nipple epidermis.[7,8] The immunohistochemical studies support this hypothesis. The presence of oncoprotein c-erbB-2 in the breast malignancy demonstrates that the staining in the underlying breast carcinoma (usually the comedo type) and Paget cells are similar. It suggests that the ductal carcinoma and Paget cells may be histologically and biologically similar.[9,10]
Another hypothesis is the theory of intraepidermal transformation; it suggests that Paget cells emerge independently in the nipple epidermis using in situ transformation into malignancy or degeneration of existing cells.[5] This hypothesis is supported by the ultrastructural studies, which have exemplified the desmosomal connections between the Paget cells and the adjacent keratinocytes. This finding is in contrast to the migratory nature of the first theory. The presence of intermediate cells with features of both Paget cells and keratinocytes supports the second hypothesis.[11,12] There are few cases of Paget disease, which only affects the epidermis of the nipple-areola, and no underlying breast cancer or tumor.
CLASSIFICATION OF PAGET’S DISEASE
Based on the presence associated with underlying breast malignancy, there are three types of Paget disease[13] [Figure 1].
Paget disease without DCIS.
Paget disease with associated DCIS within the vicinity of NAC.
Paget disease with associated DCIS or invasive carcinoma along the lactiferous ducts of the NAC and associated DCIS or invasive breast cancer elsewhere in the breast parenchyma, at least 2 cm from the nipple-areolar complex.
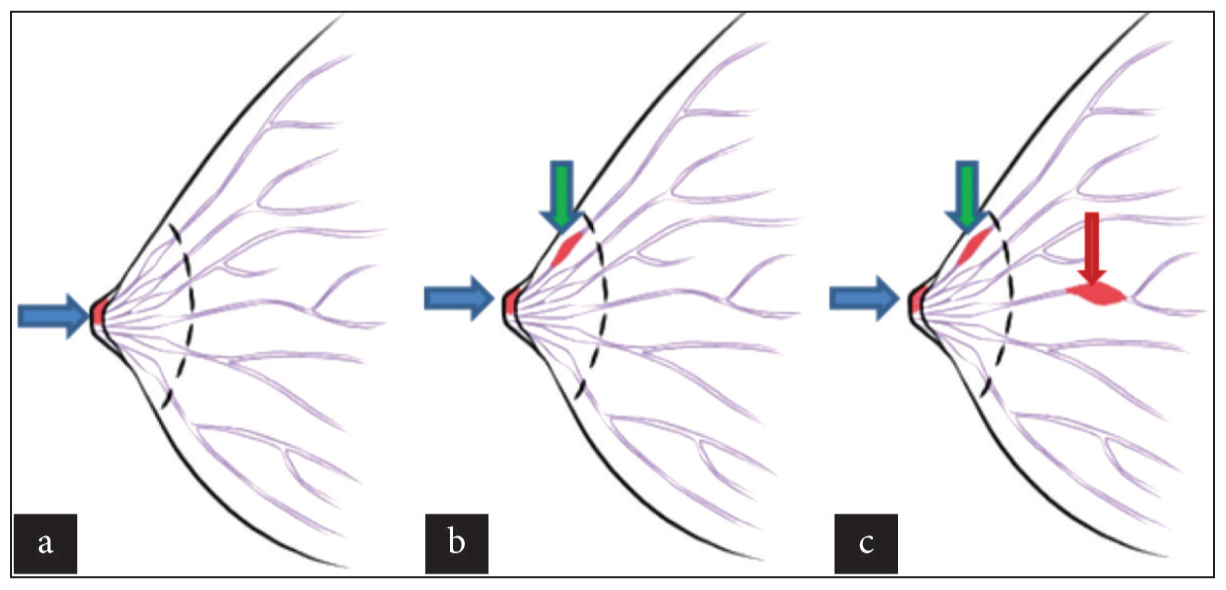
- Diagrammatic representation of the various categories of Paget’s disease. (a) Paget’s disease of nipple without DCIS (blue arrow). (b) Paget’s disease of nipple (blue arrow) with DCIS in underlying lactiferous duct (green arrow). (c) Paget’s disease of the nipple with DCIS or invasive cancer in the breast at a distant location (red arrow) (at least 2 cm from the nipple-areolar complex) involving the nipple (blue arrow), involving underlying duct (green arrow).
In one study, 104 patients with Paget disease revealed 63(60%) cases of invasive carcinoma, 34(33%) cases of DCIS, and only 7(7%) patients who detected Paget disease of the nipple without IDC or DCIS.[14] Paget disease without DCIS can be due to in situ transformation into malignancy, or it may also mean that the underlying malignancy is not large enough to be seen on imaging. This is supported by the fact that many studies demonstrated similar cases in which the associated malignancy was detected 1–2 years after diagnosing the Paget disease.[13,15,16]
Clinical Features
The clinical presentation of Paget disease is characterized by the gradual destruction of the nipple and the nipple and areola become red and covered with scales. Subsequently, the scales get detached, and the nipple gets destroyed. Complaints of itching and pain are usually associated. The nipple may be retracted or deformed in the beginning and later get replaced by a bright red weeping surface usually affects the nipple and areola; however, in the advanced stage, it may involve the surrounding skin. It is associated with a palpable mass in approx. 50% of patients.[17] Invasive cancers are more common in cases with palpable masses. However, DCIS is common in non-palpable masses.[18] Multifocal malignant lesions are observed in 42–63% of various studies.[19] Paget disease may show hyperkeratosis and parakeratosis with epidermal hyperplasia in long-standing chronic cases.[20] Paget disease of the breast may occur in men also, and clinical features are similar to those found in women. It may involve the accessory nipple or ectopic breast.[21,22] It may be asymptomatic and only diagnosed by the pathologist in the mastectomy specimen.[22] The prognosis of Paget disease is different in cases that present with palpable mass from the cases of non-palpable mass. Patients with palpable masses have a higher probability of invasive breast cancers and a higher rate of axillary lymph node metastasis.[23]
Differential Diagnosis
Both benign and malignant conditions may involve the skin of the nipple, areola, and surrounding skin. It usually presents with erythema, erosions, scaling, vesicles, ulcerations, deformity, retraction, or combinations of these features. A correct diagnosis is important because of the possibility of the underlying malignancy. Benign differential diagnoses of Paget disease are chronic eczema, dermatitis of the nipple, psoriasis, and lichen simplex chronicus. Malignant conditions involving the nipple-areolar complex are Paget disease, Bowen’s disease, basal cell carcinoma, and superficial spreading malignant melanoma.
Role of Radiology in Diagnosis
Diagnosis of Paget disease is mainly by clinical evaluation, and skin biopsy is the diagnostic standard. However, radiology plays a crucial role in the detection of associated occult malignancies in the breast. Clinical and radiological imaging features are complementary to each other. In a proven case of Paget disease, one must consider the evaluation of the breast with imaging, preferably with MRI, for the detection of associated malignancy, and it has become the standard of care before the surgical intervention.
RADIOLOGICAL FEATURES
Mammography
It is the first investigation of choice in evaluating breast diseases. Mammography evaluation is necessary in all cases with clinical suspicion of Paget disease to detect underlying malignancy, to exclude multifocal disease, and for surgical planning and follow-up in conservative treatment. Even though the mammographic features are not specific to Paget disease, one should correlate it with clinical findings.[24] On mammography, we may find the nipple changes as skin thickening, nipple retraction, malignant calcifications (clustered, amorphous, or pleomorphic), or a mass in the nipple-areolar complex region. Mammography may detect mass, architectural distortion, asymmetry, or malignant calcification in breast parenchyma. However, mammography may show normal findings despite the presence of nipple changes on clinical examination. Any non-specific findings, such as nipple-areola thickening, should be correlated with clinical findings of breast examination to confirm or exclude[25] [Figure 2]. The sensitivity of mammography to detect Paget is higher in the presence of a mass[25,26] [Figure 3]. About 29–50% of the patients with Paget disease may show normal imaging findings on mammography. If the presence of disease is seen on mammography, it may underestimate the extent of the underlying disease.[19,25] This necessitates the evaluation of the extent of the lesion with other imaging modalities, such as ultrasonography or MRI of the breast.[24] Mammography can be normal in upto 15% of patients[27] and it has been demonstrated by Morrogh et al. that 65% of these patients do have underlying cancer which was not apparent on the mammogram.[16] It is essential to evaluate the entire breast, even if the subareolar mass is detected on clinical or mammography examination due to the multicentricity of the Paget disease [Figure 4]. Use of tomosynthesis images is helpful in detecting small masses or asymmetry. Magnification views also can be used for evaluation.
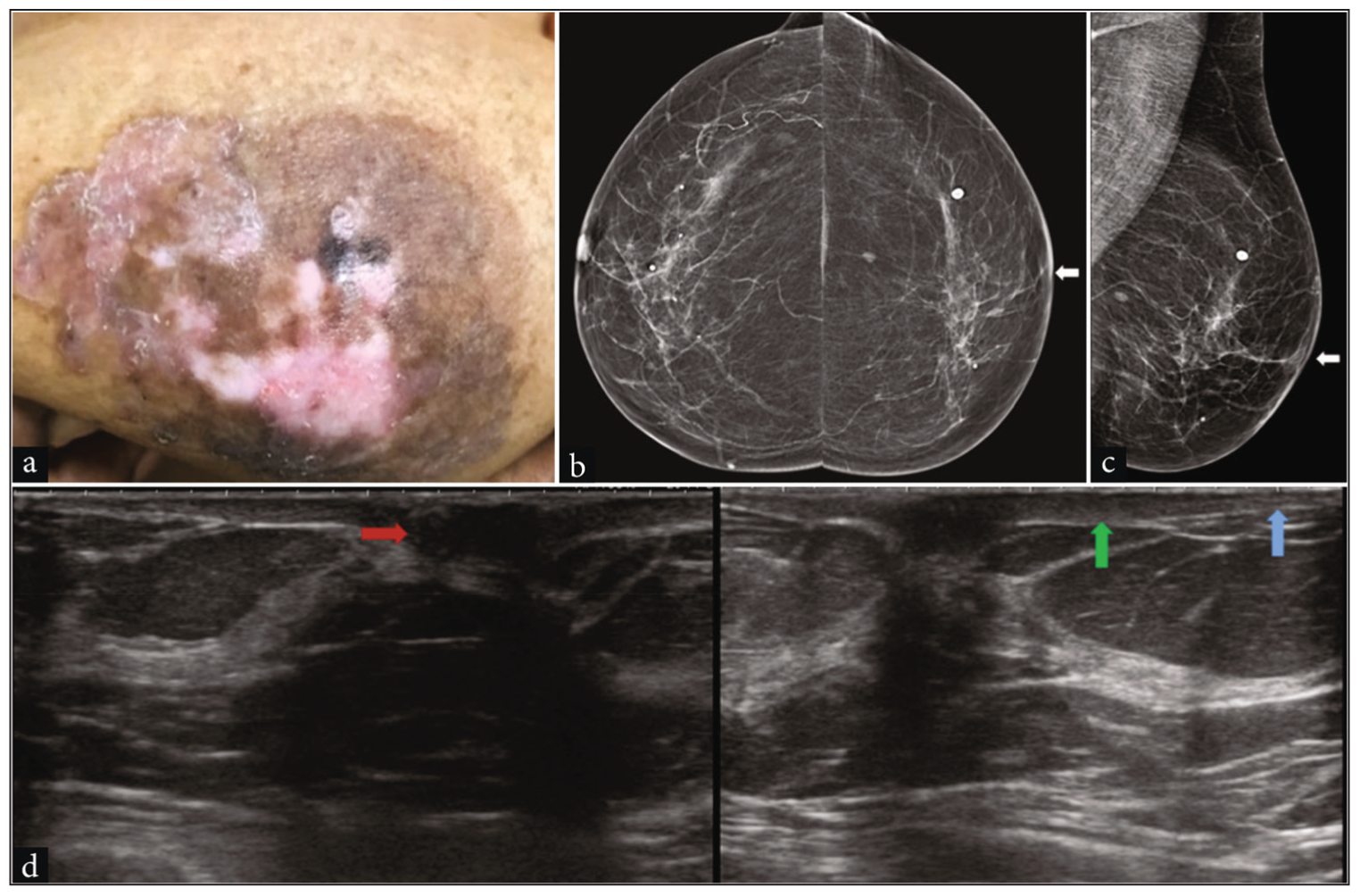
- Paget’s disease of the nipple without any abnormal mass or microcalcification in the breast parenchyma in a 62-year-old woman presented with complete erosion, discoloration of the left breast nipple with mild ulceration of the skin. (a) Clinical picture demonstrating the visible changes. (b) Digital mammogram, Craniocaudal view showing erosion of left nipple and mild thickening of nipple areolar skin (white arrow). (c) Mediolateral oblique view of left breast showing complete erosion of left breast nipple (white arrow). (d) High-resolution ultrasound of the left breast revealed a hypoechoic lesion in the nipple region with acoustic shadowing (red arrow), thickened skin of the nipple-areolar complex (green arrow), and normal skin of the rest of the breast (blue arrow).

- Paget’s disease with associated invasive ductal cancer in a 64-year-old woman who presented with a lump in left breast (a) digital mammogram Craniocaudal view and (b) a tomosynthesis image of the left breast demonstrating a retracted nipple and thick skin of the nipple-areolar complex (blue arrows) due to Paget’s disease. There is an irregular mass of invasive ductal carcinoma with spiculated margins seen in breast parenchyma (red arrows).
Ultrasonography in Paget disease
Ultrasonography should be considered in the initial evaluation of patients with negative mammographic features with high clinical suspicion. High-resolution ultrasound may demonstrate nipple changes, thickened skin, and presence of mass or calcification in the underlying breast [Figure 4], heterogeneity in the breast parenchyma, duct ectasia, or a combination of these features.[24] However, the modality is highly operator-dependent and could not detect concordant breast malignancy. Breast cancer was occult in both mammography and ultrasound in 13% of 52 cases in one study.[27]
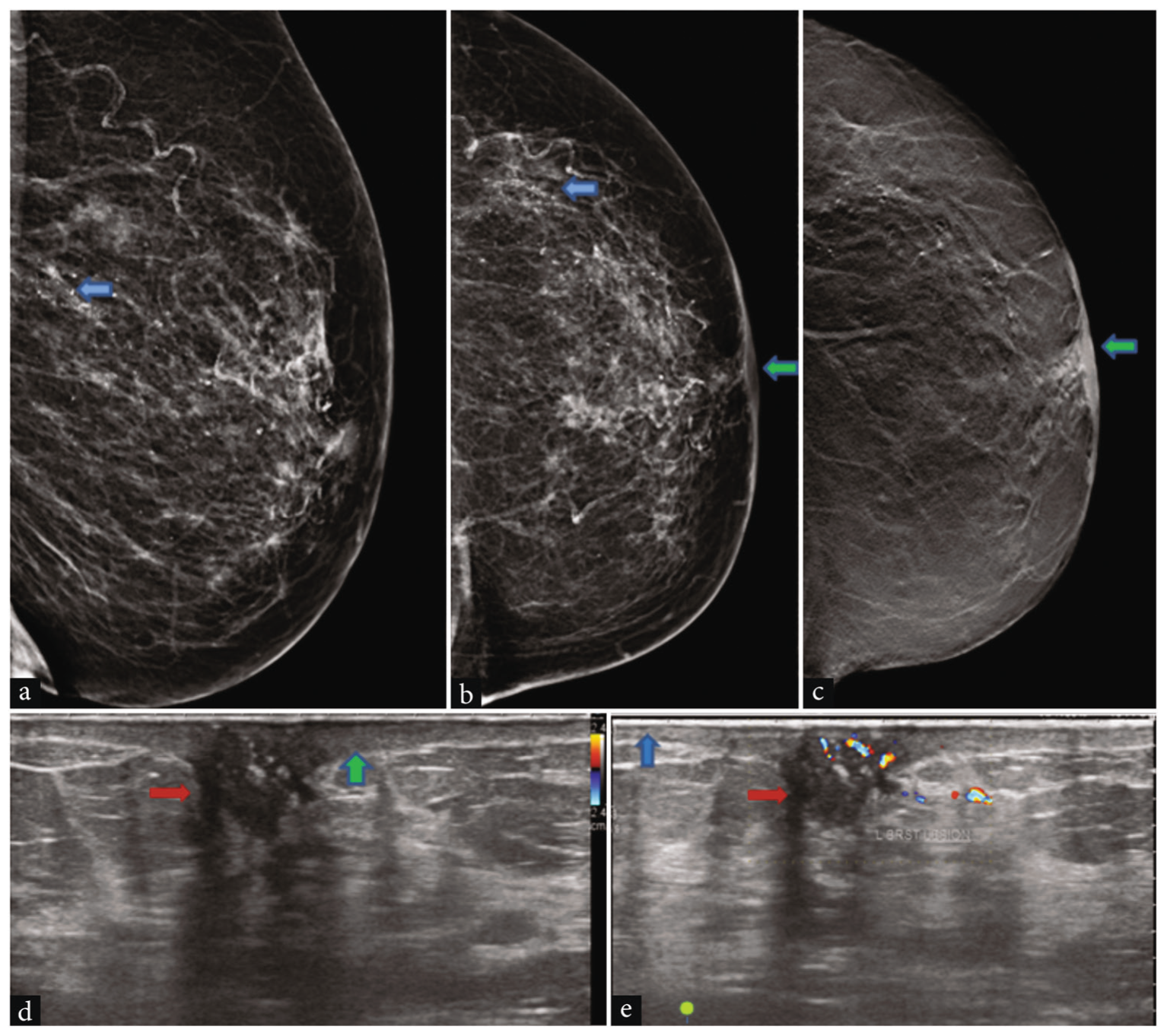
- Case of Paget’s disease with DCIS in a 60-year-old woman. Digital mammogram of the left breast (a) Mediolateral oblique, (b) Craniocaudal view, and (c) tomosynthesis image revealed microcalcification scattered in the breast (blue arrows). Erosion of the left nipple and thickening of the nipple areolar skin are seen more clearly on tomosynthesis images (green arrows). (d and e) High-resolution ultrasound and color Doppler of the left breast revealed a hypoechoic lesion in the nipple region with vascularity and acoustic shadowing (red arrows), thickened skin of the nipple areolar complex (green arrow), and normal skin of the rest of the breast (blue arrow). DCIS: Ductal carcinoma in situ.
MRI in Paget disease
MRI can be helpful in the evaluation of the nipple-areolar complex whenever there is clinical suspicion of Paget disease.[16] The role of MRI has gained immense importance in the presurgical evaluation of Paget disease of the nipple as well as the presence of underlying malignancy and its accurate extent, multifocality, and multicentricity of the lesion, especially when the other two modalities (mammography and ultrasonography) show negative results. Contrast-enhanced dynamic MRI of breasts may reveal the nipple-areolar complex edema, skin thickening, and enhancement pattern [Figure 5], retro-areolar mass, dilated ducts, enhancing mass lesion in breast parenchyma, or a combination of these findings. MRI provides a difference between the normal and abnormal nipple-areolar complex regarding deformity, erosion, enhancement, or morphology [Figure 6]. MRI has higher sensitivity to evaluate the nipple-areolar complex and overlying skin when only the epidermis is involved in Paget disease without underlying DCIS or invasive cancer. DCE-MRI can detect occult malignancy and malignancy that is at a distance from the nipple [Figure 7]. This ability of the MRI assists in patient selection for breast conservation surgery. Other than this, it also guides the biopsy of the suspected mass lesion.[24] Appropriate surgical treatment should be selected for individual patients based on radiological findings. MRI is beneficial in providing information on the involvement of the nipple-areola, their extent and distant lesions, and multiple lesions.
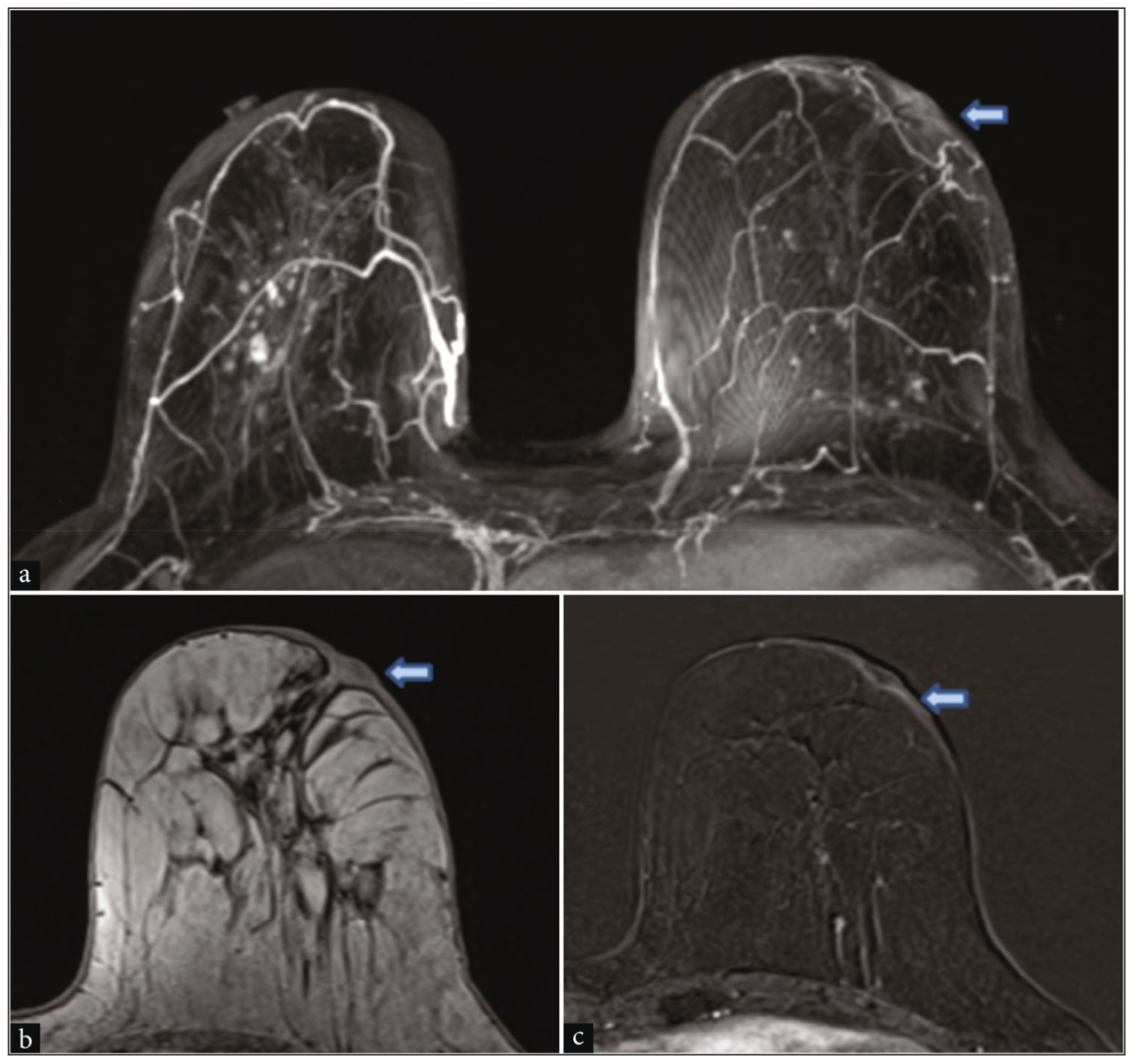
- Dynamic contrast-enhanced MRI. (a) Dynamic contrast-enhanced MRI axial maximum intensity projection revealed erosion of the left breast nipple with thickening of the overlying skin of the nipple areola (blue arrow). Right side nipple showing normal enhancement. (b) Axial T1WI without fat-suppressed image showing thickening of the skin (blue arrow). (c) Post-contrast subtracted image showing mild enhancement of the nipple areolar region (blue arrow).
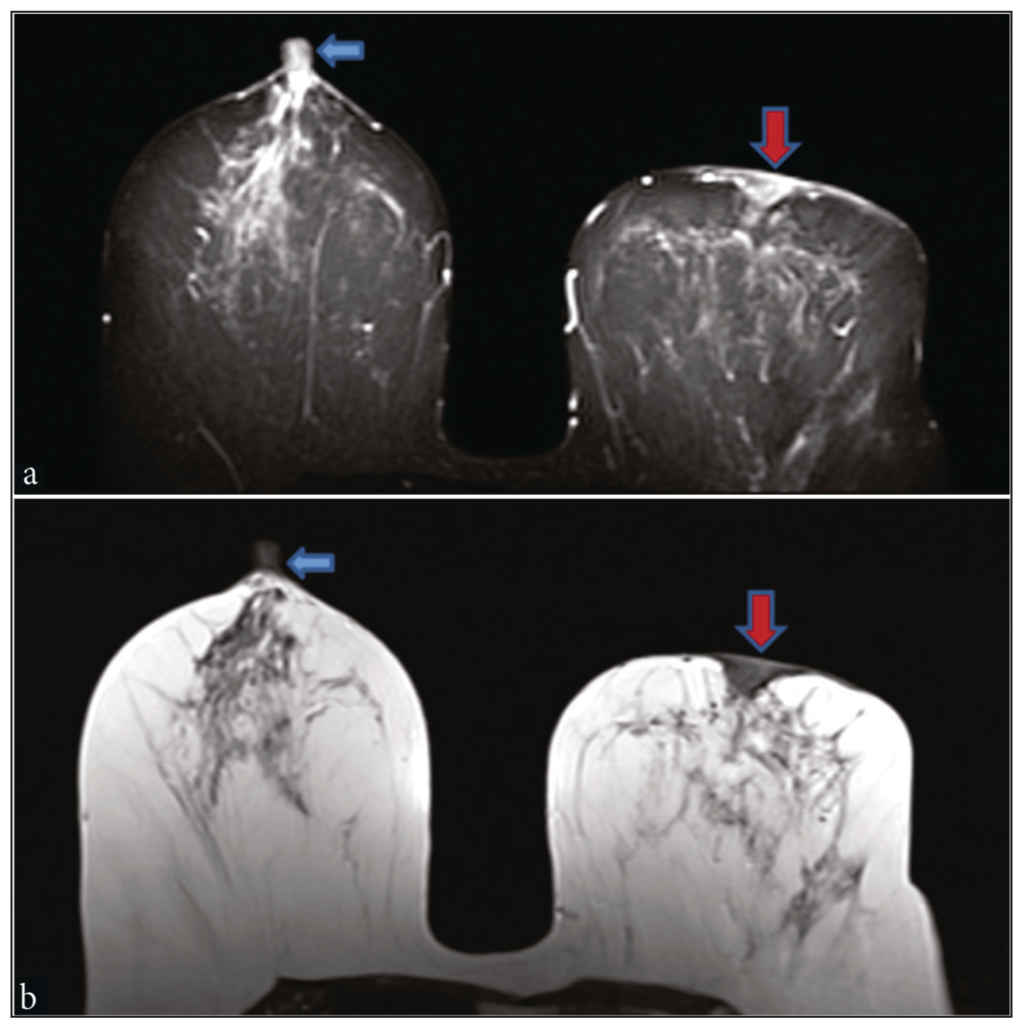
- Case of Paget’s disease. (a) Short tau inversion recovery axial MRI revealed erosion of the left breast nipple and edema in the nipple areolar region (red arrow), and the right side nipple was normal (blue arrow). (b) Non-fat suppressed axial T2WI image showing erosion and thickening of skin over left nipple (red arrow); right nipple is normal (blue arrow).
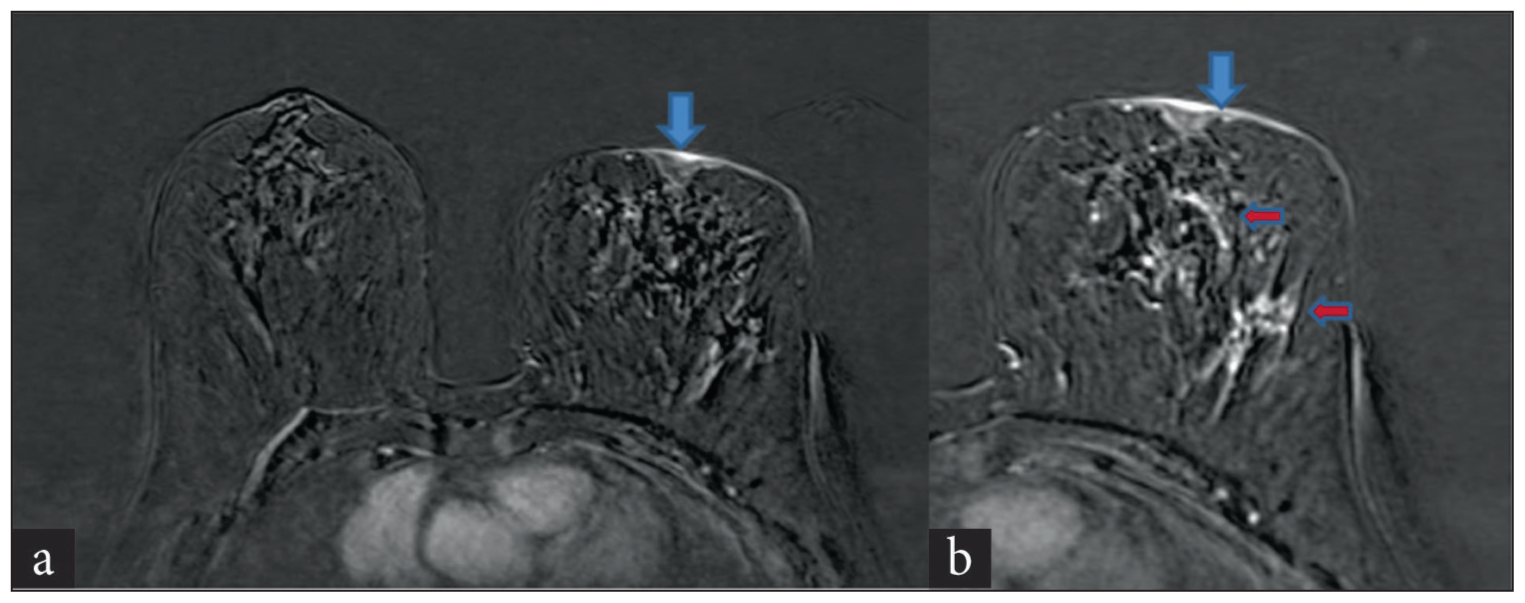
- (a) Case of Paget’s disease with DCIS—dynamic contrast-enhanced MRI revealed erosion of the left breast nipple and abnormal enhancement in the nipple areolar region (blue arrow), with the right side nipple showing normal enhancement. (b) Erosion of nipple and abnormal enhancement (blue arrow), few areas of non-mass enhancement seen in breast parenchyma (red arrows). DCIS: Ductal carcinoma in situ.
Pathology
Paget disease of the nipple characterizes invasion of the epidermis by Paget cells. Paget cells are large, pale-staining cells with round or oval nuclei and large nucleoli between the normal keratinocytes of the nipple epidermis. Paget cells spread into the lactiferous sinuses under the nipple and then invade the overlying epidermis of the nipple. Epidermis may be eroded or hyperplastic.[18] The cells possess microscopic features of glandular cells which are positive for the oncogene HER2/neu, suggesting common genetic alterations for both the epidermal and breast tumor cells. A negative result does not exclude Paget’s disease, and in clinical suspicion, a surgical biopsy should be considered.[20]
CURRENT MANAGEMENT RECOMMENDATIONS FOR PAGET DISEASE
The current recommendation is breast conservation surgery, which involves wide local excision of the nipple and areola to achieve clear margins, complete resection of the associated mass lesion if any are present, staging of axillary nodes, and radiation therapy. Earlier, total mastectomy with or without axillary dissection was considered a standard treatment.[19,28] The survival rates were similar in both cases; they were comparable; however, the size of the underlying mass lesion and the presence of metastatic axillary lymph nodes act as independent prognostic factors for survival.[29] All the patients who are considered for breast-conservation surgery should undergo presurgical evaluation with MRI breast, and all these patients should be followed up routinely after the surgery.[24] For many patients, breast conservative surgery and irradiation provide an acceptable management and cosmetic appearance and obviate mastectomy and breast reconstruction. Nipple-areolar reconstruction can be performed 4–6 months after the radiation therapy. For patients considering conservative surgery, thorough preoperative evaluation is suggested to rule out occult multicentric disease, and these patients should be regularly followed up by regular mammography.
CONCLUSION
All patients with any nipple complaints that are suspicious of Paget disease should undergo systematic clinical, radiological, and pathological evaluation for the planning of management. Although Paget disease is primarily a clinical diagnosis, a negative mammogram or MRI cannot exclude an underlying cancer. Diagnosis of Paget disease requires careful clinical examination and radiologic and histopathological findings. Clinical and imaging findings complement each other to confirm the diagnosis or exclude the possibility of Paget disease.
Ethical approval
The Institutional Review Board has waived the ethical approval for this study.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- On the disease of the mammary areola preceding cancer of the mammary gland. St Bartholomews Hosp Rep. 1874;10:87-9.
- [Google Scholar]
- Paget’s disease of the breast: The experience of the European Institute of Oncology and review of the literature. Breast Cancer Res Treat. 2008;112:513-21.
- [CrossRef] [PubMed] [Google Scholar]
- Mammary and extramammary Paget’s disease. J Eur Acad Dermatol Venereol. 2007;21:581-90.
- [Google Scholar]
- Pathogenesis and treatment of Paget’s disease of the breast. Cancer. 1981;48:825-9.
- [CrossRef] [PubMed] [Google Scholar]
- Paget’s disease of the breast: What the radiologist may expect to find. Aust Radiol. 1995;39:27-30.
- [Google Scholar]
- Histogenesis of extramammary and mammary Paget cells: An immunohistochemical study. Am Dermatopathol. 1989;11:313-8.
- [CrossRef] [PubMed] [Google Scholar]
- Paget’s disease of the skin: A unifying concept of histogenesis. Cancer. 1982;50:2203-6.
- [Google Scholar]
- An immunohistochemical study of the presence of c-erbB-2 protein in Paget’s disease of the nipple. Histopathology. 1989;15:505-14.
- [Google Scholar]
- c-erbB-2 oncoprotein expression in mammary and extramammary Paget’s disease: An immunohistochemical study. Histopathology. 1990;17:243-7.
- [CrossRef] [PubMed] [Google Scholar]
- Paget’s disease of the nipple: Alternative management in cases without or with minimal extent of underlying breast carcinoma. Cancer. 1984;54:545-51.
- [CrossRef] [PubMed] [Google Scholar]
- Ultrastructural observations on epidermal cells in Paget’s disease of the breast. Am J Pathol. 1969;57:49-64.
- [Google Scholar]
- Paget disease of the breast: Findings at magnetic resonance imaging and histopathologic correlation. Invest Radiol. 2005;40:363-7.
- [CrossRef] [PubMed] [Google Scholar]
- Paget’s disease of the breast: There is a role for breast-conserving therapy. Ann Surg Oncol.. 2005;12:391-7.
- [CrossRef] [PubMed] [Google Scholar]
- Significance of nipple enhancement of Paget’s disease in contrast enhanced breast MRI. Arch Gynecol Obstet. 2010;282:157-62.
- [CrossRef] [PubMed] [Google Scholar]
- MRI identifies otherwise occult disease in select patients with Paget disease of the nipple. J Am Coll Surg. 2008;206:316-21.
- [Google Scholar]
- Paget disease of the nipple: A multifocal manifestation of higher-risk disease. Cancer. 2002;95:1-7.
- [Google Scholar]
- Paget’s disease of the ectopic breast with an underlying intraductal carcinoma: Report of a case. J Cutan Pathol. 1986;13:59-66.
- [CrossRef] [PubMed] [Google Scholar]
- Paget’s disease of the breast: A 33-year experience. J Am Coll Surg. 1998;187:171-7.
- [CrossRef] [PubMed] [Google Scholar]
- Paget disease of the breast: Mammographic, US, and MR imaging findings with pathologic correlation. RadioGraphics. 2011;31:1973-7.
- [CrossRef] [PubMed] [Google Scholar]
- Paget disease of the nipple: Radiologic-pathologic correlation. Radiology. 1993;189:89-94.
- [Google Scholar]
- Mammographic appearances in Paget’s disease of the breast. Clin Radiol. 1994;49:185-8.
- [Google Scholar]
- Paget’s disease of the breast: Clinical, mammographic, sonographic and pathologic findings in 52 cases. Eur J Radiol. 2006;60:256-63.
- [CrossRef] [PubMed] [Google Scholar]
- The conservative management of Paget’s disease of the breast with radiotherapy. Cancer. 1997;80:1065-72.
- [CrossRef] [PubMed] [Google Scholar]
- Paget disease of the breast: Changing patterns of incidence, clinical presentation and treatment in the U.S. Cancer. 2006;107:1448-58.
- [CrossRef] [PubMed] [Google Scholar]




