

Translate this page into:
A clinical study to assess safety profile of adjuvant hypo-fractionated radiation therapy of 1 week duration in the management of early-stage breast carcinoma

*Corresponding author: Natasha Laishram, Department of Radiation Oncology, Vydehi Institute of Medical Sciences and Research Centre, Bangalore, India. laishramnatasha@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Laishram N, Vishwanathan B, Narayanan GS. A clinical study to assess safety profile of adjuvant hypo-fractionated radiation therapy of 1 week duration in the management of early-stage breast carcinoma. Indian J Breast Imaging. doi: 10.25259/IJBI_19_2024
Abstract
Objectives
Breast cancer is the most common cancer in women both worldwide and in India. In India, it comprised 27.70% of all new cancer cases in females in 2018 and caused 12.11% of cancer deaths, amounting to 87,0901. The crude rate of projected incidence of cancer statistics in India, 2020, for breast cancer in females is 1 in 29, and the annual percentage change in age-adjusted incidence rates over the period 1982–2014 was 3.1% in Bangalore. So far there are scarce Indian studies on extreme hypofractionation. Hence, the study was taken up.
Materials and Methods
Thirty patients with post-operative early breast cancer who required adjuvant RT were selected for this study. 26 Gy in 5 fractions were delivered to the PTV chest wall/breast tissue with a sequential lumpectomy boost to a dose of 10 Gy in 5 fractions in post-BCS cases by the 3DCRT technique. Patients were clinically evaluated and toxicities graded as per RTOG. Acute and late toxicity criteria at baseline, at the completion of radiation therapy, 3 weeks, 3 months, and 6 months post-radiation therapy for skin and subcutaneous changes. 2D echo, CT chest were done at the baseline and also at post-treatment at 3 months and 6 months to note any cardiac or lung changes.
Results
The majority of the patients had no skin or subcutaneous reactions. Grade I skin reaction was seen in 3 patients at the end of RT and another 3 patients at 3 weeks post RT among those who received sequential boost in post-BCS patients. Grade I subcutaneous reaction was seen in 4 patients at 3 months and 6 patients at 6 months. Sonomammogram was done on follow-up at 3 months and 6 months post-RT showing mild inflammatory changes in 5 patients at 3 months and fibrosis in 1 patient at 3 and 6 months who had received whole breast RT with tumor bed boost (19 patients). Grade I cardiac toxicity was seen in 1 patient at 6 months post RT. The patient had received NACT followed by MRM followed by adjuvant RT to the left chest wall. 2DECHO done before the start of RT and 3 months post-RT was normal. At 6 months post-RT, it showed minimal pericardial effusion with 57% left ventricular ejection fraction (Grade I cardiac toxicity according to RTOG toxicity). However, the patient was asymptomatic.
Conclusion
Extreme hypofractionation of 26 Gy in 5 fractions post-MRM or post-BCS with sequential tumor bed boost in the adjuvant setting of early-stage breast cancer post-systemic therapy is well tolerated. However, a longer follow-up is required for assessment of overall survival, disease-free survival, and further late toxicity profile in a large multi-institutional setting, recruiting a larger number of patient populations to confirm the present clinical findings.
Keywords
Adjuvant RT
Early breast carcinoma
Extreme hypofractionation

INTRODUCTION
Breast carcinoma is the most common cancer in women both worldwide and in India. The GLOBOCAN 2018[1] shows the age-standardized incidence of the disease worldwide to be 25.8 per 100,000 population. However, in India, it comprised 27.7% of all new cancers in females in 2018 and caused 12.11% of all cancer deaths. It is also the second highest cause of cancer associated with DALY in India.[1] The crude rate of projected incidence of cancer statistics in India in 2020 for breast cancer in females was 1 in 29, and the annual percentage change in age-adjusted incidence rate (AAR) over the period 1982–2014 was 3.1% in Bengaluru.[2]
The prolonged treatment schedule of breast carcinoma consisting of surgery, chemo/hormone therapy, and radiation therapy can be shortened by using a short duration of radiation therapy instead of a long duration without much change in the survival rate.
Breast carcinoma radiation schedules have traditionally followed the fractionated schedule of 50 Gy in 25 fractions over 5 weeks. Hypofractionation refers to a radiation therapy regimen in which a higher dose per fraction of radiation is delivered over a shorter total treatment period, compared to conventional fractionation. This approach is increasingly used for treating breast cancer due to its effectiveness, safety, and convenience. Hypofractionated radiation therapy has been increasingly adopted worldwide after the publication of mature data from the START trial[3] and Canadian trials.[4] These trials have shown a non-inferiority result of hypofractionation to that of conventional fractionation in early-stage breast carcinoma. Extreme hypofractionation is a type of radiotherapy fractionation where very high doses per fraction are delivered over a significantly shortened treatment duration, typically in 1 week. So far there are scarce Indian studies on extreme hypofractionation. Hence, the study was undertaken.
MATERIALS AND METHODS
The study is a single-arm, prospective, interventional, hospital-based study carried out from February 2021 to July 2022. The Institutional Ethical Committee clearance (ethics number ECR/747/Inst/KA/2015/RR-18) was obtained before the start of the study. Thirty patients who fulfilled the inclusion criteria were treated with 3D conformal radiation therapy (3DCRT) technique.
Inclusion criteria: Postmastectomy or postbreast conservative surgery (BCS) patients requiring radiotherapy after informed written consent.
pT1-3, N0, M0
Age: 18–65 years
Eastern Cooperative Oncology Group (ECOG) performance status: 0–2.
Exclusion criteria
Metastatic breast carcinoma
Prior RT to thorax or palliative RT
Serious medical or psychiatric illness
Patient with either supraclavicular or internal mammary or axillary lymph node-positive either clinically or radiologically or on sentinel lymph node biopsy.
Target volumes: Planning target volume was contoured according to Radiation Therapy Oncology Group (RTOG) guideline of breast/chest wall radiation therapy.[5] PTV target volume for tumor bed boost was delineated 0.5 cm from surgical clips. A total tumor dose of 26 Gy in 5 fractions over 1 week to the whole breast or chest wall was delivered to the PTV. Sequential conformal tumor boost 10 Gy in 5 fractions in all post-BCS patients.
The patients were clinically evaluated, and toxicities were graded as per RTOG. Acute and late toxicity criteria at baseline, at completion of radiation therapy, 3 weeks, 3 months, and 6 months postradiation therapy for skin and subcutaneous changes. 2D Echo, computed tomography (CT) chest was done at the baseline and also at posttreatment at 3 months and 6 months to note any cardiac or pulmonary changes.
Plan evaluation: PTV → V90% ≥ 95%
V107% ≤ 2% of PTV
Ipsilateral lung dose V8 Gy < 15%
Heart dose V7 Gy < 5%
All of the patients achieved the planning dosimeters.
Statistical Analysis
Data were entered into a Microsoft Excel data sheet and were analyzed using SPSS 22 version software. Categorical data were represented in the form of frequencies and proportions. Continuous data were represented as mean and standard deviation. Graphical representation of data: MS Excel and MS Word were used to obtain various types of graphs, such as bar diagrams and pie diagram. A P-value of < 0.05 was considered as statistically significant after assuming all the rules of statistical tests.
Observations
Thirty patients with early breast carcinoma were recruited for the study. Seventeen patients had right-sided tumors (56.7%), and 13 patients had left-sided tumor (43.3%); the mean age was 46 years (range 40–60 years). Twenty of the patients had upper outer quadrant tumor (66.7%), seven of them in the lower outer quadrant (23.3%); two patients had tumor in upper inner quadrant (6.7%), and one patient had a lower inner quadrant tumor (3.3%) [Table 1]. ER and PR positivity was seen in 17 of the patients (56.7%); HER2 was positive in seven patients (23.3%), eight patients (26.6%) were triple-negative breast cancer. Neoadjuvant chemotherapy (NACT) was given, consisting of four cycles of Adriamycin (60 mg/m2), Cyclophosphamide (600 mg/m2) followed by four cycles of Paclitaxel (175 mg/m2) at the standard doses (given at 3 weekly intervals) in 11 (36.7%) of the cases, followed by surgery, while 19 (63.3%) patients received adjuvant chemotherapy of the same regimen following surgery and anti-Her2Neu targeted therapy (3 weekly Injection Trastuzumab 8 mg/kg week 1 followed by 6 mg/kg to complete 1 year of therapy) was given for patients with Her2Neu positive (23.3%). Nineteen patients (63.3%) of the patients underwent breast conservation surgery (BCS) + sentinel lymph node biopsy (SLNB) followed by standard chemotherapy as given in the NACT setting [Table 2]. All the patients were treated with external beam radiation therapy (EBRT) with 6 MV energy with 3D conformal radiation therapy (3DCRT technique) giving 26 Gy in 5 fractions. All patients who underwent BCS received tumor bed boost of 10 Gy in 5 fractions. None of the patients received nodal radiotherapy. Three patients (10%) were of Stage IIIA (cT3N0M0, pT3N0) with Luminal A type. Hence, nodal RT was not given.
| N = 30 | % | ||
| Quadrant of primary tumor | LIQ | 1 | 3.3 |
| LOQ | 7 | 23.3 | |
| UIQ | 2 | 6.7 | |
| UOQ | 20 | 66.7 | |
| Total | 30 | 100.0 | |
LIQ: Lower inner quadrant, LOQ: Lower outer quadrant, UIQ: Upper inner quadrant, UOQ: Upper outer quadrant.
| Quadrant of primary tumor | N = 30 | % | |
| Clinical group staging (preoperative) | IIA | 11 | 36.7 |
| IIB | 16 | 53.4 | |
| IIIA | 3 | 10 | |
| Surgery | BCS+SLNB | 19 | 63.3 |
| MRM+ALND | 8 | 26.7 | |
| MRM+SLNB | 3 | 10 | |
| Pathological group stage (postoperative) | 0 | 5 | 16.7 |
| IA | 2 | 6.7 | |
| IIA | 19 | 63.3 | |
| IIB | 4 | 13.3 | |
BCS: Breast conservation surgery, SLNB: Sentinel lymph node biopsy, MRM: Modified radical mastectomy, ALND: Axillary lymph node dissection.
RESULTS
The present study enrolled thirty patients with early breast cancer from February 2021 to July 2022, and patients were followed up for a period of 6 months post-RT (radiation therapy). On assessing clinically, three patients (10%) had Grade I skin reaction on Day 5 of RT. Three weeks post-RT, another three patients (10%) had Grade I skin reaction. Three months post-RT, four patients (13.3%) had Grade I subcutaneous fibrosis. Six months post-RT, six patients (0.30%) had Grade I subcutaneous fibrosis. Sonomammogram done on follow-up at 3 months and 6 months post-RT showed mild inflammatory changes in five patients (6.7%) at 3 months [Figure 1]. Subcutaneous fibrosis was seen radiologically (sonomammogram) in 1 (3.3%) patient at 3 and 6 months who had received whole breast RT with tumor bed boost (19 patients). All patients had normal sonomammographic findings on the opposite breast at 3 months and 6 months follow-up post-RT. The majority of the patients with abnormal sonomammographic findings at 3 months had a preceding Grade I skin reaction at 3 weeks post-RT [Figure 2].
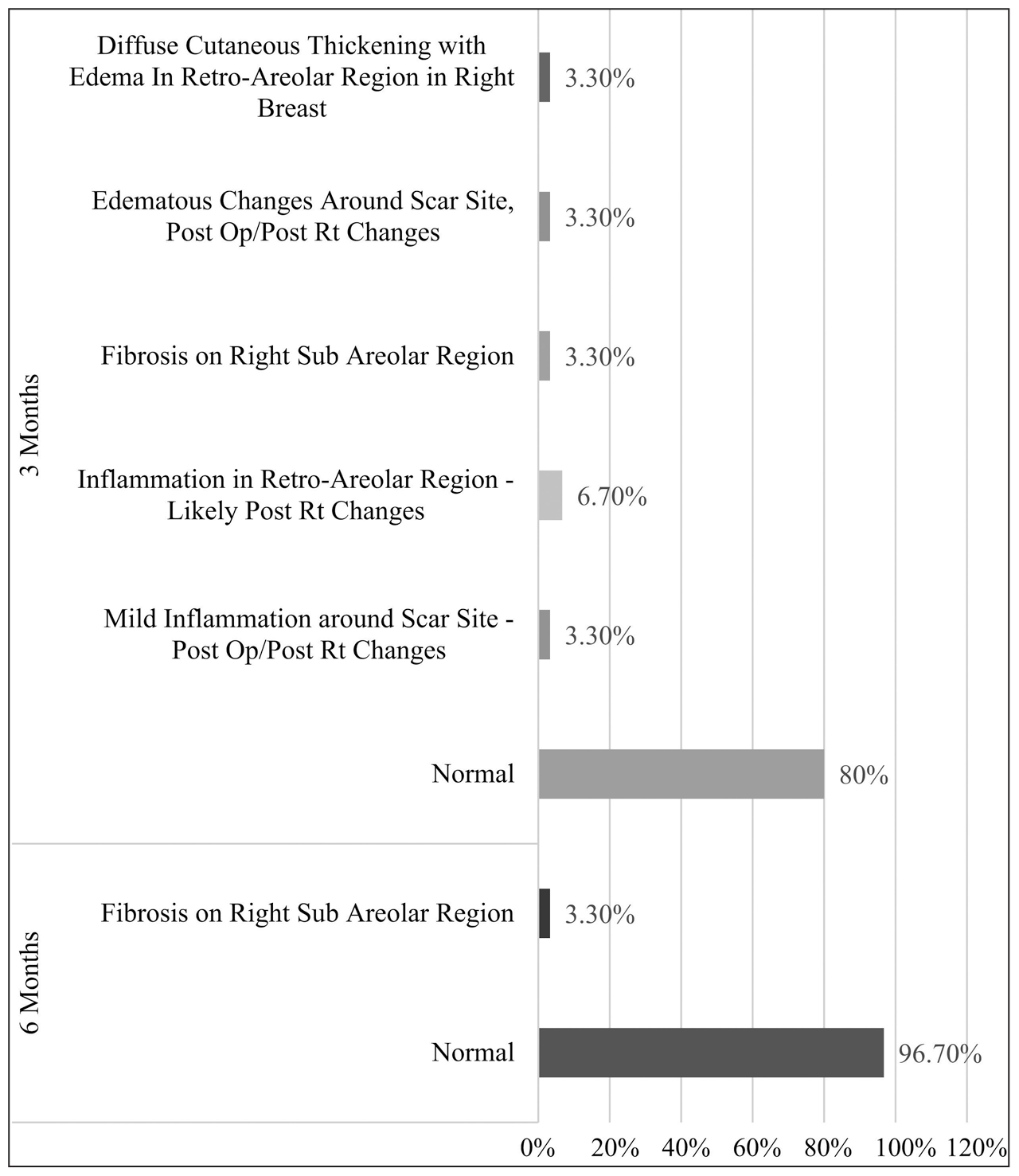
- Bar graph showing sonomammography findings post-RT. Op: Operative, Rt: Radiotherapy.
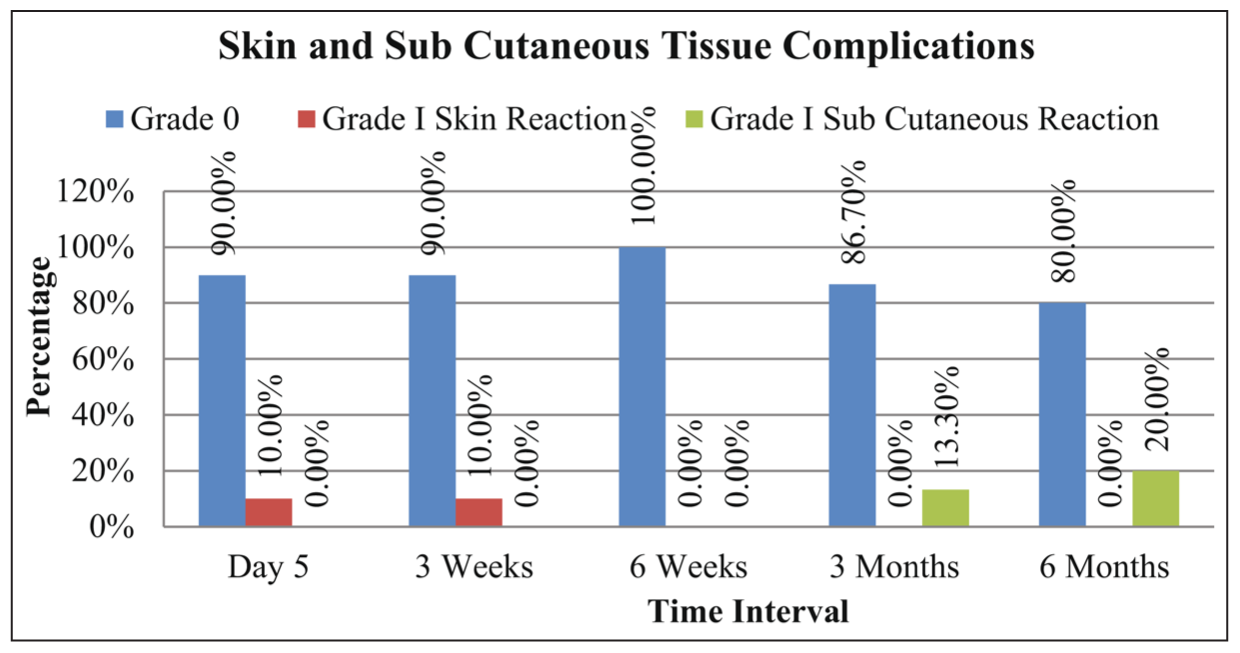
- Bar graph showing skin and subcutaneous tissue toxicities on clinical examination.
In the present study, one patient had asymptomatic Grade I pericardial effusion at 6 months post-RT. This patient had received four cycles of NACT followed by MRM + ALND followed by adjuvant RT to the Left chest wall. 2DECHO done before the start of RT and 3 months post-RT was normal. At 6 months post-RT, it showed minimal pericardial effusion with 57% left ventricular ejection fraction (Grade I cardiac toxicity according to RTOG toxicity). However, the patient was asymptomatic. The patient was Her2Neu negative. However, she received NACT with four cycles of Adriamycin and Cyclophosphamide. Whether the pericardial effusion that developed was due to Adriamycin or RT remains inconclusive.
DISCUSSION
Breast cancer RT schedules have traditionally followed conventionally fractionated RT of 50 Gy in a 25-fraction regimen to the chest wall and whole breast. Fractionation changes started with the matured data of the START trial[3] and Canadian trials. [4] The use of hypofractionated regimens was infrequent and was part of institutional practice in very few centers worldwide. This practice has changed since the past few years, after the publication of mature data from the START trial[3] and Canadian trials.[4] There have been a growing number of studies[3,4,6–11] attempting to decrease the overall treatment time for RT after surgery and systemic therapy through the administration of fewer but larger daily doses of RT delivered to the whole breast or only to the portion of the breast containing the primary tumor, including the chest wall.
Several prospective randomized trials demonstrated that the hypofractionated RT is noninferior to the conventional fractionated RT with respect to treatment outcomes and toxicities after surgery and systemic therapy.[12,13]
The 10-year follow-up results of the hypofractionated radiation therapy for breast cancer trial conducted by Whelan et al. in 2000 (Canadian trial)[4] showed a comparably good or excellent cosmetic outcome (71.3% in the conventional fractionated arm as compared to 69.8% in hypofractionated arm with a 95% confidence interval of −6.9 to 9.8). In the FAST-Forward trial,[6] longitudinal analysis of all annual clinical assessments of normal tissue effects over follow-up for 5 years showed a significantly increased risk of any moderate or marked effect in the breast or chest wall for the 27 Gy in 5 fraction group compared with 40 Gy in 15 fraction (OR 1.55, p < 0.0001), with no significant difference between 26 Gy in 5 fraction and 40 Gy in 15 fraction (moderate normal tissue effect 9.9%, 15.4%, 11.9%, respectively, for 40 Gy, 27 Gy, and 26 Gy group; breast shrinkage was seen in 5.5%, 8.2%, 6.8%, respectively, for 40 Gy, 27 Gy, and 26 Gy group). This was similar for the individual effects of breast distortion, shrinkage, induration, and breast or chest wall edema, with a significantly higher risk for 27 Gy than 40 Gy but not for 26 Gy. It also showed a significantly higher risk of moderate or marked breast hardness or firmness for 27 Gy compared with 40 Gy (OR 1.42, p = 0.0003) and a lower risk of change in breast appearance for 26 Gy compared with 27 Gy (p = 0.0018), but no significant differences between schedules for the other normal tissue effects. Twenty-seven percent of the patients receiving 26 Gy had Grade II acute skin reaction as compared to 55% of the patients receiving 40 Gy. Grade III–IV acute skin reaction was seen more in the 40 Gy group as compared to 26 Gy group (14% vs. 6%). Thirty-six percent of the patients receiving 26 Gy had Grade I late skin reaction as compared to 51% on the 40 Gy group.[8] A comparable outcome was also seen in the present study, with the majority Grade I acute skin toxicity observed mostly in patients receiving tumor bed boost in post-BCS patients. Grade I early and late subcutaneous reactions were also observed in patients who received tumor bed boost in post-BCS patients. The findings in our study were also comparable with the study conducted by Nugent et al.[14] which included early-stage breast carcinoma postsurgery treated with adjuvant radiation therapy of 26 Gy in 5 fractions with sequential tumor bed boost for post-BCS cases. The study showed that almost half of the patients had Grade I skin reactions and no grade 3 and above skin toxicities were seen. Comparing 26 Gy in 5 fractions with and without a boost, Grade 0 toxicity was higher in the boost group (29% vs. 17%), while Grade 1 was more common in the non-boost group (52% vs. 35%). Grade 2 toxicity rates were similar (30% vs. 35%). Faint erythema (Grade 1) was the most frequent acute effect, occurring in 44% of patients in week 1 and persisting in 27% by week 4. Grade 2 toxicity, including breast edema, peaked at 20% in week 1 and decreased to 3% by week 4, indicating manageable and predominantly low-grade acute skin reactions. A study conducted by Sigaudi et al.[15], which included treatment of early breast cancer with 26 Gy in 5 fractions, showed grade 2 erythema (6.7%), grade 2 induration (4.4%), and grade 2 skin color changes.
Of 27 patients with a cardiac-related death in the FAST Forward trial,[7] 15 had a history of cardiac disease reported at randomization or were a current or ex-smoker in the past year. In our present study, Grade I asymptomatic pericardial effusion was seen in one patient at 6 months post-RT. This patient had received four cycles of NACT followed by MRM + ALND followed by adjuvant RT to the left chest wall. 2DECHO done before the start of RT and 3 months post-RT was normal. At 6 months post-RT, it showed minimal pericardial effusion with 57% left ventricular ejection fraction (Grade I cardiac toxicity according to RTOG toxicity). The patient was Her2Neu negative. However, she received NACT with four cycles of Adriamycin and Cyclophosphamide. Whether the pericardial effusion that developed was due to Adriamycin or RT remains inconclusive.
Strengths
The strengths of the study include its prospective design, use of standardized 3DCRT technique, and focus on extreme hypofractionation (26 Gy in 5 fractions), particularly relevant in the Indian context where such data is limited. The detailed assessment of acute and late toxicities and the use of imaging for cardiac and pulmonary evaluation enhance its rigor. The study demonstrates hypo-fractionated radiotherapy as a safe, effective, and convenient treatment option for early breast cancer.
Limitations
Our limitations include a small sample size of 30 patients and a short follow-up duration of 6 months, which limits the evaluation of long-term outcomes, late toxicities, and recurrence rates. Being a single-center study, its findings lack generalizability to other settings. The absence of a control arm prevents direct comparison with conventional fractionation. Additionally, the study does not assess quality of life or patient-reported outcomes, and toxicity evaluation relied on subjective clinical grading, introducing potential observer bias. Long-term cardiac and pulmonary effects were also insufficiently explored. Larger, multi-center trials with longer follow-up and comprehensive evaluations are needed to validate these findings.
CONCLUSION
In conclusion, extreme hypofractionation of 26 Gy in 5 fractions post-MRM and post-BCS cases with sequential tumor bed boost in the adjuvant setting of early-stage breast cancer post-systemic therapy is well tolerated. However, a longer follow-up is required for assessment of overall survival, disease-free survival, and further late toxicity profile in a large multi-institutional setting, recruiting a larger number of patient populations to confirm the present clinical finding.
Ethical approval
The research/study approved by the Institutional Review Board at Vydehi Institute of Medical Sciences & Research Centre, number ECR/747/Inst/KA/2015/RR-18, dated 12th February 2021.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394-424.
- [CrossRef] [PubMed] [Google Scholar]
- The global burden of disease study 1990–2016. Lancet Oncol. 2018;19:1289-306.
- The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomized controlled trials. Lancet Oncol. 2013;14:1086-94.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term results of hypo-fractionated radiation therapy for breast cancer. N Engl J Med. 2010;362:513-20.
- [CrossRef] [PubMed] [Google Scholar]
- Consistency of ESTRO and RTOG contouring guidelines for target volume delineation in early stage breast cancer. Int J Radiol Radiat Ther. 2020;7:133-40.
- [CrossRef] [Google Scholar]
- The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: A randomised trial. Lancet. 2008;371:1098-107.
- [CrossRef] [PubMed] [Google Scholar]
- Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial. Lancet. 2020;395:1613-26.
- [CrossRef] [PubMed] [Google Scholar]
- Acute skin toxicity associated with a 1-week schedule of whole breast radiotherapy compared with a standard 3-week regimen delivered in the UK FAST-Forward Trial. Radiother Oncol. 2006;7:467-71.
- [CrossRef] [PubMed] [Google Scholar]
- Dose-escalated simultaneous integrated boost radiotherapy in early breast cancer (IMPORT HIGH): A multicentre, phase 3, non-inferiority, open-label, randomised controlled trial. Lancet. 2023;401:2124-37.
- [CrossRef] [PubMed] [Google Scholar]
- Partial-breast radiotherapy after breast conservation surgery for early breast cancer (UK IMPORT LOW trial): 5-year results from a multicentre, randomised, controlled, phase 3, non-inferiority trial. Lancet. 2017;390:1048-60.
- [CrossRef] [PubMed] [Google Scholar]
- Hypofractionated versus standard fractionated radiotherapy in patients with early breast cancer or ductal carcinoma in situ in a randomized phase III trial: The DBCG HYPO trial. J Clin Oncol. 2020;38:3615-25.
- [CrossRef] [PubMed] [Google Scholar]
- Hypofractionated versus conventional fractionated postmastectomy radiotherapy for patients with high-risk breast cancer: A randomised, non-inferiority, open-label, phase 3 trial. Lancet Oncol. 2019;20:352-60.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: Long-term results of a randomised trial. Lancet Oncol. 2006;7:467-71.
- [CrossRef] [PubMed] [Google Scholar]
- Implementation of 26 Gy in five fractions over 1-week adjuvant radiotherapy for breast cancer: Prospective report of acute skin toxicity and consideration of resource implications. Breast. 2023;67:55-61.
- [CrossRef] [PubMed] [Google Scholar]
- Ultra-hypofractionation for whole-breast irradiation in early breast cancer: Interim analysis of a prospective study. Biomedicines. 2022;10:2568.
- [CrossRef] [PubMed] [Google Scholar]




