

Translate this page into:
Impact of multidisciplinary discussions on the management of breast diseases
*Corresponding author: Manisha Bahl, Department of Radiology, Massachusetts General Hospital/Harvard Medical School, Boston, USA. mbahl1@mgh.harvard.edu
-
Received: ,
Accepted: ,
How to cite this article: Bahl M. Impact of multidisciplinary discussions on the management of breast diseases. Indian J Breast Imaging. 2025;3:3–6. doi: 10.25259/IJBI_16_2025
INTRODUCTION
Multidisciplinary care refers to the coordinated collaboration of specialists to provide evidence-based and personalized treatment plans that are tailored to each patient’s needs. For the management of breast cancer, multidisciplinary discussions, which include radiologists, pathologists, surgeons, medical oncologists, and radiation oncologists, are essential for synthesizing clinical, imaging, and pathological findings and developing comprehensive treatment plans. In addition to cancer management, multidisciplinary input can also be valuable in guiding care for patients with high-risk breast lesions and those with ambiguous or discordant biopsy results. Input from multiple experts helps determine appropriate follow-up or intervention and can reduce the risk of both over- and under-treatment.
COMPREHENSIVE BREAST CANCER MANAGEMENT THROUGH MULTIDISCIPLINARY COLLABORATION
Multidisciplinary cancer conferences, also referred to as multidisciplinary team meetings, multidisciplinary case management meetings, or tumor boards, are collaborative forums in which specialists meet in person or virtually to discuss care for patients diagnosed with cancer.[1] These teams typically include radiologists, pathologists, surgeons, medical oncologists, radiation oncologists, and nurses. The goal of multidisciplinary cancer conferences is to integrate clinical, imaging, and pathological data to develop consensus-driven, evidence-based management plans. In fact, a recent meta-analysis found that patients with breast cancer whose cases had been discussed at multidisciplinary cancer conferences had significantly better survival outcomes compared to those managed without such input (hazard ratio, 0.68; 95% confidence interval, 0.48–0.94).[2]
An important component of multidisciplinary evaluation in breast cancer care is the accurate assessment of disease extent, which involves correlating findings from imaging with biopsy results. Extent of disease informs the selection of neoadjuvant or adjuvant therapies, surgical planning, and eligibility for breast-conserving surgery. In my practice, decisions regarding the need for contrast-enhanced breast MRI to assess the extent of disease are often made during the multidisciplinary cancer conference [Figure 1]. Indications for MRI may include premenopausal status; postmenopausal status with triple-negative breast cancer, human epidermal growth factor receptor 2-positive tumors, or invasive lobular carcinoma; known genetic mutations or high-risk status; eligibility evaluation for accelerated partial breast irradiation; size discrepancy greater than 1 cm between clinical exam, mammography, and ultrasound; suspected multifocal or multicentric disease; and assessment for neoadjuvant chemotherapy.[3]

- A 46-year-old woman with ductal carcinoma in situ (DCIS) of the right breast. The patient was recalled from screening mammography to further evaluate calcifications in the right breast. (a) Craniocaudal magnification view of the right breast shows grouped pleomorphic calcifications in the upper outer quadrant (white circle). Stereotactic biopsy was performed, yielding grade 2 DCIS. During the multidisciplinary cancer conference, the decision was made to obtain a pre-operative MRI examination given the patient’s premenopausal status. (b) Post-contrast fat-saturated T1-weighted axial image from the breast MRI shows non-mass enhancement in the upper outer quadrant of the right breast (white arrow), corresponding to the known malignancy. (c) Post-contrast fat-saturated T1-weighted axial image shows an enhancing mass in the upper outer quadrant of the left breast (white circle). Ultrasound-guided core needle biopsy of the mass yielded grade 2 invasive ductal carcinoma. The patient subsequently underwent bilateral nipple-sparing mastectomies.
Similar to the multidisciplinary cancer conference, multidisciplinary clinics, which are also referred to as multidisciplinary rounds, one-stop clinics, or multidisciplinary committees, bring together specialists who work together, often in a single setting, to deliver coordinated and streamlined care.[1] These clinics provide patients with a complete evaluation and unified treatment recommendations during a single visit. In one study conducted at an academic institution in the United States, patients with stage II or III breast cancer evaluated in a same-day multidisciplinary clinic had a significantly shorter median time to initiation of neoadjuvant chemotherapy compared to those seen through traditional, sequential consultations (12.7 days versus 24.4 days, p < 0.001).[4] Multidisciplinary clinics have been shown to improve the efficiency of care and the timeliness of treatment, particularly for patients who require prompt therapeutic intervention.
INDIVIDUALIZED MANAGEMENT OF HIGH-RISK BREAST LESIONS
High-risk breast lesions, also referred to as B3 lesions or lesions of uncertain malignant potential, represent a heterogeneous group of lesions with two associated risks. First, high-risk lesions can be upgraded to breast cancer at the time of surgical excision. Second, high-risk lesions confer an increased long-term risk of developing breast cancer. Historically, women with high-risk lesions diagnosed by image-guided biopsy routinely underwent surgical excision to evaluate for an associated malignancy. However, accumulating evidence has shown that the upgrade risk for many of these lesions is relatively low, particularly in the setting of radiology-pathology concordance. This evidence has led to a growing trend toward conservative management and surveillance. In fact, the American Society of Breast Surgeons now acknowledges that surveillance may be appropriate for certain high-risk lesions, including atypical ductal hyperplasia (ADH), particularly when the lesion is small, well-sampled, and radiology-pathology concordant.[5]
In clinical practice, multidisciplinary conferences can play a valuable role in guiding individualized management of women diagnosed with high-risk breast lesions. These discussions include input from breast imaging radiologists, pathologists, surgeons, and other breast specialists who together review the patient’s clinical history, imaging findings, biopsy technique, and pathological features. Management recommendations are made based on a combination of these variables. For example, focal ADH involving one to two terminal duct lobular units, with more than 90% of targeted calcifications removed during stereotactic biopsy, may lead to a recommendation for imaging surveillance, formal risk assessment, and counseling about risk reduction.[6] In contrast, the presence of a mass on imaging, limited sampling of the target lesion (<50%), or extensive atypia raises greater concern for underestimation and typically results in a recommendation for surgical excision. Patients managed through such multidisciplinary pathways are closely followed over time.
MULTIDISCIPLINARY REVIEW OF DISCORDANT OR INDETERMINATE BIOPSY RESULTS
Image-guided biopsies, which are widely used to evaluate suspicious breast lesions, are highly accurate and considered to be a cost-effective alternative to surgical biopsy. However, despite their reliability, false-negative results and sampling errors can still occur. Achieving radiology-pathology (rad-path) concordance is therefore essential to confirm that biopsy results accurately reflect the imaging finding [Figure 2]. In many clinical settings, this assessment is performed independently by radiologists. However, in cases of diagnostic uncertainty or potential discordance, a multidisciplinary conference involving both radiologists and pathologists can be considered to improve diagnostic accuracy and guide optimal management.
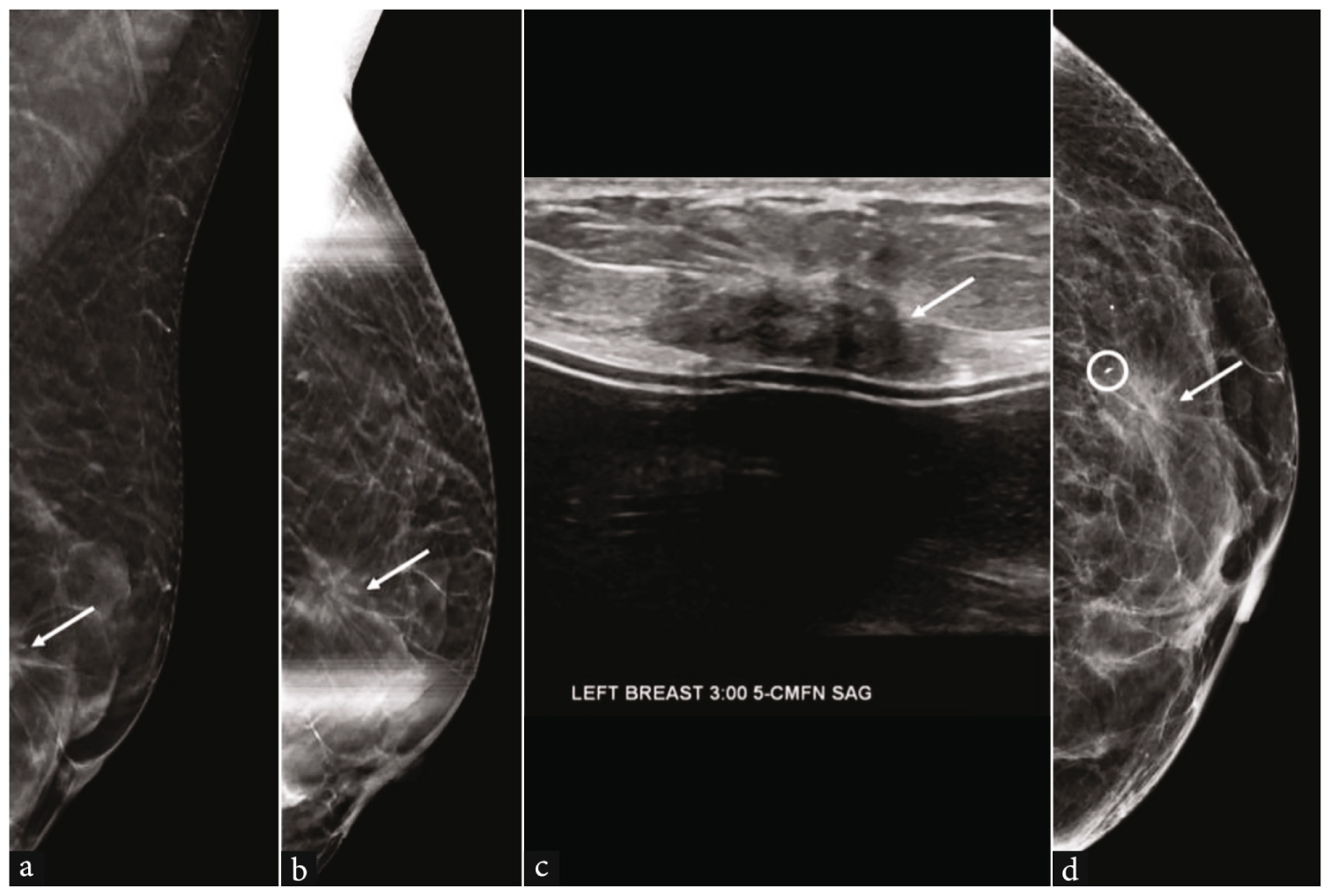
- A 64-year-old woman with invasive ductal carcinoma (IDC) of the left breast. (a) Implant-displaced mediolateral oblique tomosynthesis image from the screening mammogram shows a mass in the left breast (white arrow), which is incompletely visualized. (b) Spot compression mediolateral oblique tomosynthesis image more completely shows the mass (white arrow). (c) Targeted ultrasound demonstrates a corresponding irregular hypoechoic mass in the left breast at 3 o’clock (white arrow). The mass was biopsied under ultrasound guidance. (d) Post-procedure mammogram shows that the biopsy marker (white circle) is located at the periphery of the mass (white arrow). The biopsy pathology result was benign breast tissue, which was deemed to be discordant. Stereotactic biopsy was subsequently performed, yielding grade 1 IDC.
In a retrospective review of 4,714 image-guided breast biopsies over a 4-year period, 29.4% of cases were submitted for review at a weekly radiology-pathology correlation conference.[7] Of these, 5.3% resulted in a change in assessment or management following the conference. Specifically, the multidisciplinary discussion led to recommendations for repeat biopsy or surgical excision in 23 cases, avoided surgery in 29 cases, prevented unnecessary short-interval imaging in 22 cases, and identified cancer in three cases that might have otherwise been missed. The study authors concluded that incorporating a weekly multidisciplinary case conference into breast care practices improves cancer detection, facilitates timely identification of discordant cases, and reduces unnecessary imaging and surgical procedures.
CONCLUSION
Multidisciplinary discussions have become an important component of modern breast cancer care, providing a structured and collaborative infrastructure for treatment planning. Their benefits, however, extend beyond individual case management. At the institutional level, multidisciplinary discussions promote the standardization of care, strengthen communication among healthcare providers, and reduce variability in clinical decision-making. These meetings also serve an educational role by providing trainees and junior physicians with exposure to discussions among specialists and their clinical reasoning. From the patient perspective, multidisciplinary care can enhance trust and satisfaction by delivering coordinated, unified recommendations and minimizing delays associated with fragmented consultations.
While multidisciplinary discussions are most often associated with breast cancer treatment, their value extends to other clinical scenarios encountered by breast imaging radiologists, including the management of high-risk lesions and cases involving ambiguous or discordant biopsy results. By integrating insights from radiologists, pathologists, surgeons, oncologists, and other specialists, multidisciplinary discussions improve diagnostic accuracy, prevent unnecessary interventions, and support timely, personalized care plans. As breast care continues to evolve, driven by advances in imaging technology, artificial intelligence, genomics, and precision medicine, the multidisciplinary model will remain central to delivering high-quality, patient-centered care. To fully realize its potential, continued investment in data integration, technological infrastructure, and systematic outcome tracking will be important to further refine these collaborative practices and extend their benefits across diverse healthcare settings.
REFERENCES
- Multidisciplinary care of breast cancer patients: A scoping review of multidisciplinary styles, processes, and outcomes. Curr Oncol. 2019;26:e385-97.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- The impact of multidisciplinary cancer conferences on overall survival: A meta-analysis. J Natl Cancer Inst. 2024;116:356-69.
- [Google Scholar]
- Preoperative breast MRI: Current evidence and patient selection. J Breast Imaging. 2023;5:112-24.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of 1-day multidisciplinary clinic on breast cancer treatment. Breast Cancer Res Treat. 2020;182:623-9.
- [Google Scholar]
- 2024 [Accessed 15 May 2025]. Available from: https://www.breastsurgeons.org/docs/statements/asbrs-rg-high-risk-lesions.pdf
- Multidisciplinary considerations in the management of high-risk breast lesions. AJR Am J Roentgenol. 2012;198:W132-40.
- [CrossRef] [PubMed] [Google Scholar]
- Improving patient care by incorporation of multidisciplinary breast radiology-pathology correlation conference. Can Assoc Radiol J. 2016;67:122-9.
- [CrossRef] [PubMed] [Google Scholar]




